

Cardiovascular Manifestations From Therapeutic Radiation: A Multidisciplinary Expert Consensus Statement From the International Cardio-Oncology Society
- PMID: 34604797
- PMCID: PMC8463721
- DOI: 10.1016/j.jaccao.2021.06.003
Cardiovascular Manifestations From Therapeutic Radiation: A Multidisciplinary Expert Consensus Statement From the International Cardio-Oncology Society
Abstract
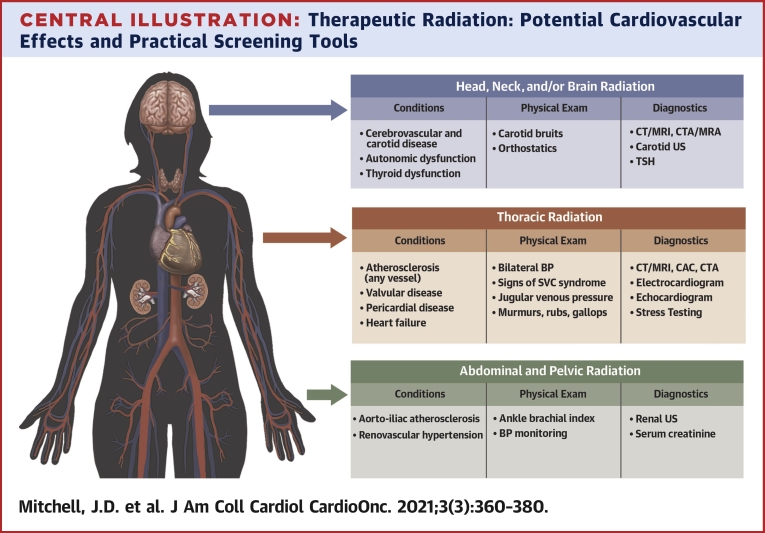
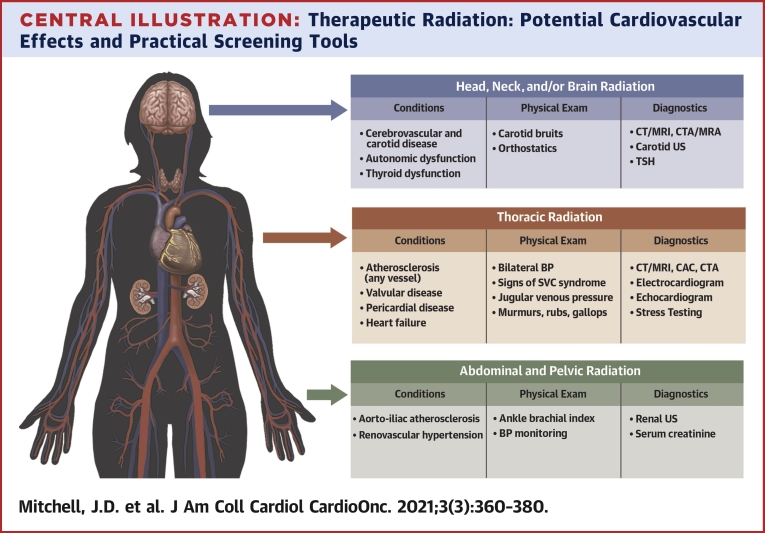
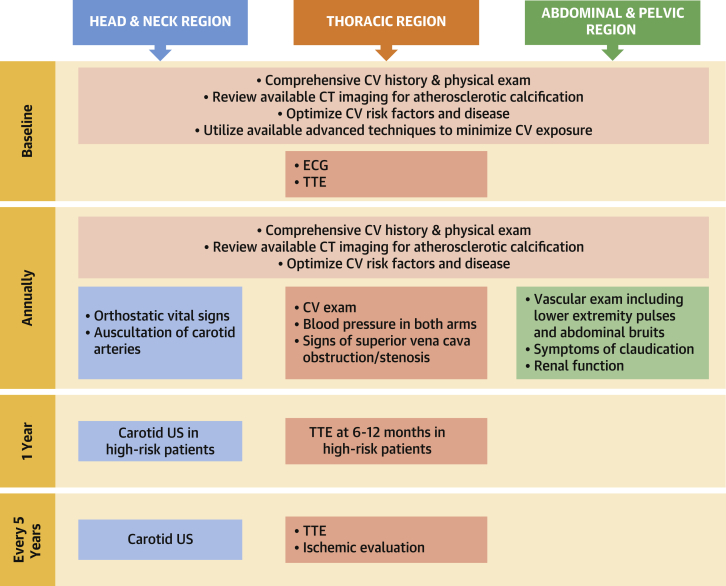
Radiation therapy is a cornerstone of cancer therapy, with >50% of patients undergoing therapeutic radiation. As a result of widespread use and improved survival, there is increasing focus on the potential long-term effects of ionizing radiation, especially cardiovascular toxicity. Radiation therapy can lead to atherosclerosis of the vasculature as well as valvular, myocardial, and pericardial dysfunction. We present a consensus statement from the International Cardio-Oncology Society based on general principles of radiotherapy delivery and cardiovascular risk assessment and risk mitigation in this population. Anatomical-based recommendations for cardiovascular management and follow-up are provided, and a priority is given to the early detection of atherosclerotic vascular disease on imaging to help guide preventive therapy. Unique management considerations in radiation-induced cardiovascular disease are also discussed. Recommendations are based on the most current literature and represent a unanimous consensus by the multidisciplinary expert panel.
Keywords: CABG, coronary artery bypass graft; CAC, coronary artery calcium; CAD, coronary artery disease; CI, confidence interval; CT, computed tomography; CTCA, computed tomography coronary angiography; CV, cardiovascular; DIBH, deep inspiratory breath hold; HF, heart failure; HL, Hodgkin lymphoma; HNC, head and neck cancer; HR, hazard ratio; LIMA, left internal mammary artery; MRI, magnetic resonance imaging; NT-proBNP, N-terminal pro–B-type natriuretic peptide; OR, odds ratio; PAD, peripheral arterial disease; RT, radiation therapy; SAVR, surgical aortic valve replacement; SVC, superior vena cava; TAVR, transcatheter aortic valve replacement; TTE, transthoracic echocardiogram; aHR, adjusted hazard ratio; cancer; cardiovascular disease; imaging; prevention; radiation therapy; screening.
© 2021 The Authors.
Conflict of interest statement
Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002345 as well as by the National Institutes of Health grant R01 HL147884. Dr Mitchell has received research funding from Pfizer, Longer Life Foundation, and Children’s Discovery Institute; and is a consultant for Pfizer (modest). Dr Bergrom has received research support from the Susan G. Komen Foundation and Innovation Pathways. Dr Ferencik has received research support from the National Institutes of Health and the American Heart Association; and is a consultant for Biograph, Inc (unrelated to current work). Dr Szmit has received personal fees from Amgen, Angelini, AstraZeneca, Bayer, Berlin-Chemie, Bristol Myers Squibb, Clinigen, Janssen-Cilag, Pfizer, Polpharma, Roche, and TEVA. Dr Zaha has received support from the Cancer Prevention Research Institute of Texas (RP180404). Dr Herrmann was supported by the National Cancer Institute of the National Institutes of Health (CA233610), the Miami Heart Foundation, and the Mayo Clinic. Dr Nohria has received research funding from Amgen, Inc; and is a consultant for Takeda Oncology and AstraZeneca. Dr Lenihan has received research funding from Myocardial Solutions; and is a consultant for Lilly, Prothena, AstraZeneca, Roche, Clementia, and Eidos (all consultancy renumeration is modest). Dr Dent has received research funding from Novartis; and is a consultant for Novartis and Eli Lilly. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Darby S.C., Ewertz M., McGale P., et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368:987–998. - PubMed
-
- van Nimwegen F.A., Schaapveld M., Cutter D.J., et al. Radiation dose-response relationship for risk of coronary heart disease in survivors of Hodgkin lymphoma. J Clin Oncol. 2016;34:235–243. - PubMed
-
- Atkins K.M., Rawal B., Chaunzwa T.L., et al. Cardiac radiation dose, cardiac disease, and mortality in patients with lung cancer. J Am Coll Cardiol. 2019;73:2976–2987. - PubMed
-
- Hull M.C., Morris C.G., Pepine C.J., Mendenhall N.P. Valvular dysfunction and carotid, subclavian, and coronary artery disease in survivors of Hodgkin lymphoma treated with radiation therapy. JAMA. 2003;290:2831–2837. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
