

Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults : A Retrospective Observational Study
- PMID: 34606315
- PMCID: PMC9012609
- DOI: 10.7326/M21-1456
Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults : A Retrospective Observational Study
Erratum in
-
Correction: Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults.Ann Intern Med. 2021 Dec;174(12):1780. doi: 10.7326/L21-0661. Ann Intern Med. 2021. PMID: 34929132 No abstract available.
Abstract
Background: There are 2 approaches to intensifying antihypertensive treatment when target blood pressure is not reached, adding a new medication and maximizing dose. Which strategy is better is unknown.
Objective: To assess the frequency of intensification by adding a new medication versus maximizing dose, as well as the association of each method with intensification sustainability and follow-up systolic blood pressure (SBP).
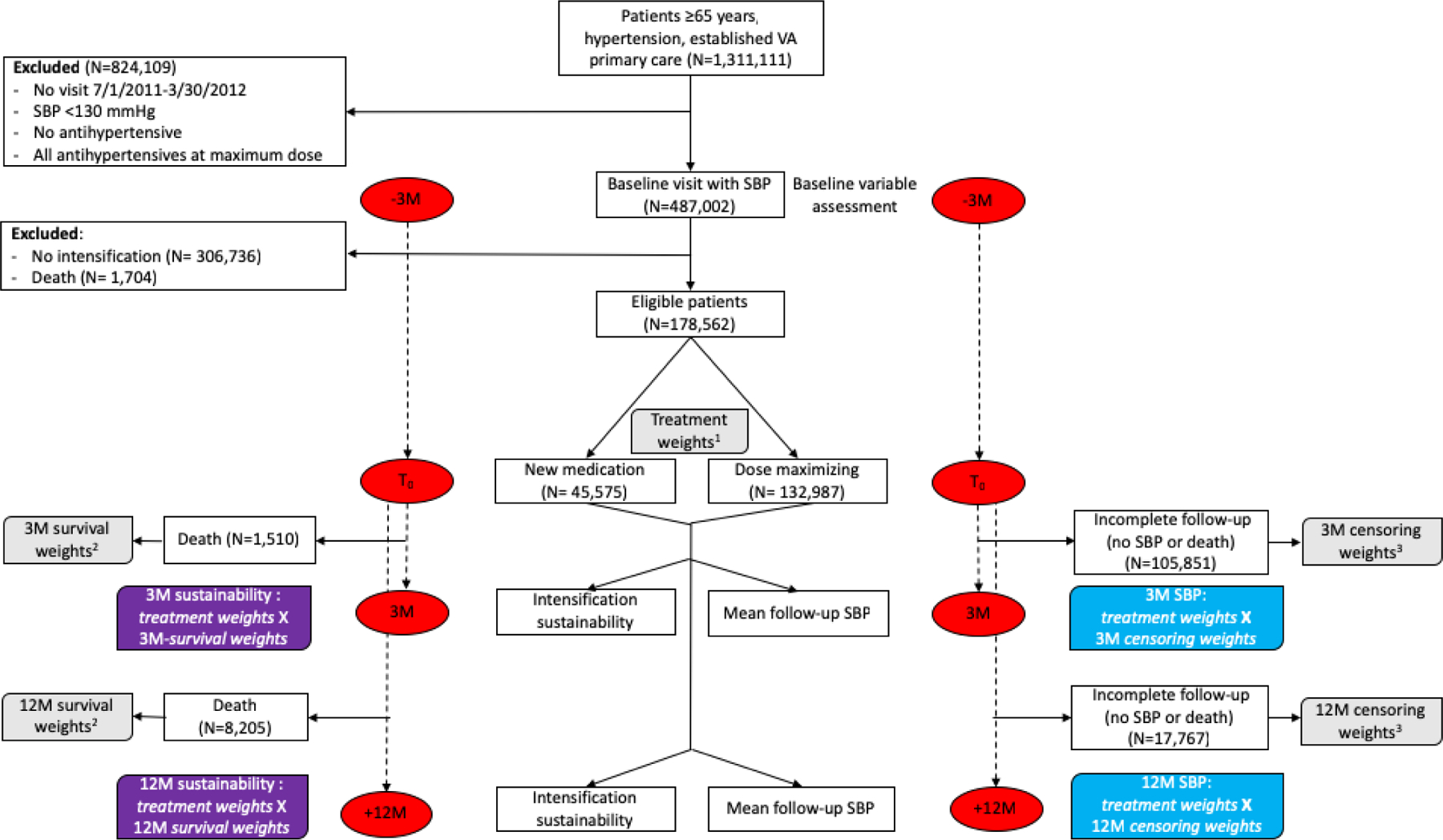
Design: Large-scale, population-based, retrospective cohort study. Observational data were used to emulate a target trial with 2 groups, new medication and maximizing dose, who underwent intensification of their drug regimen.
Setting: Veterans Health Administration (2011 to 2013).
Patients: Veterans aged 65 years or older with hypertension, an SBP of 130 mm Hg or higher, and at least 1 antihypertensive medication at less than the maximum dose.
Measurements: The following 2 intensification approaches were emulated: adding a new medication, defined as a total dose increase with new medication, and maximizing dose, defined as a total dose increase without new medication. Inverse probability weighting was used to assess the observational effectiveness of the intensification approach on sustainability of intensified treatment and follow-up SBP at 3 and 12 months.
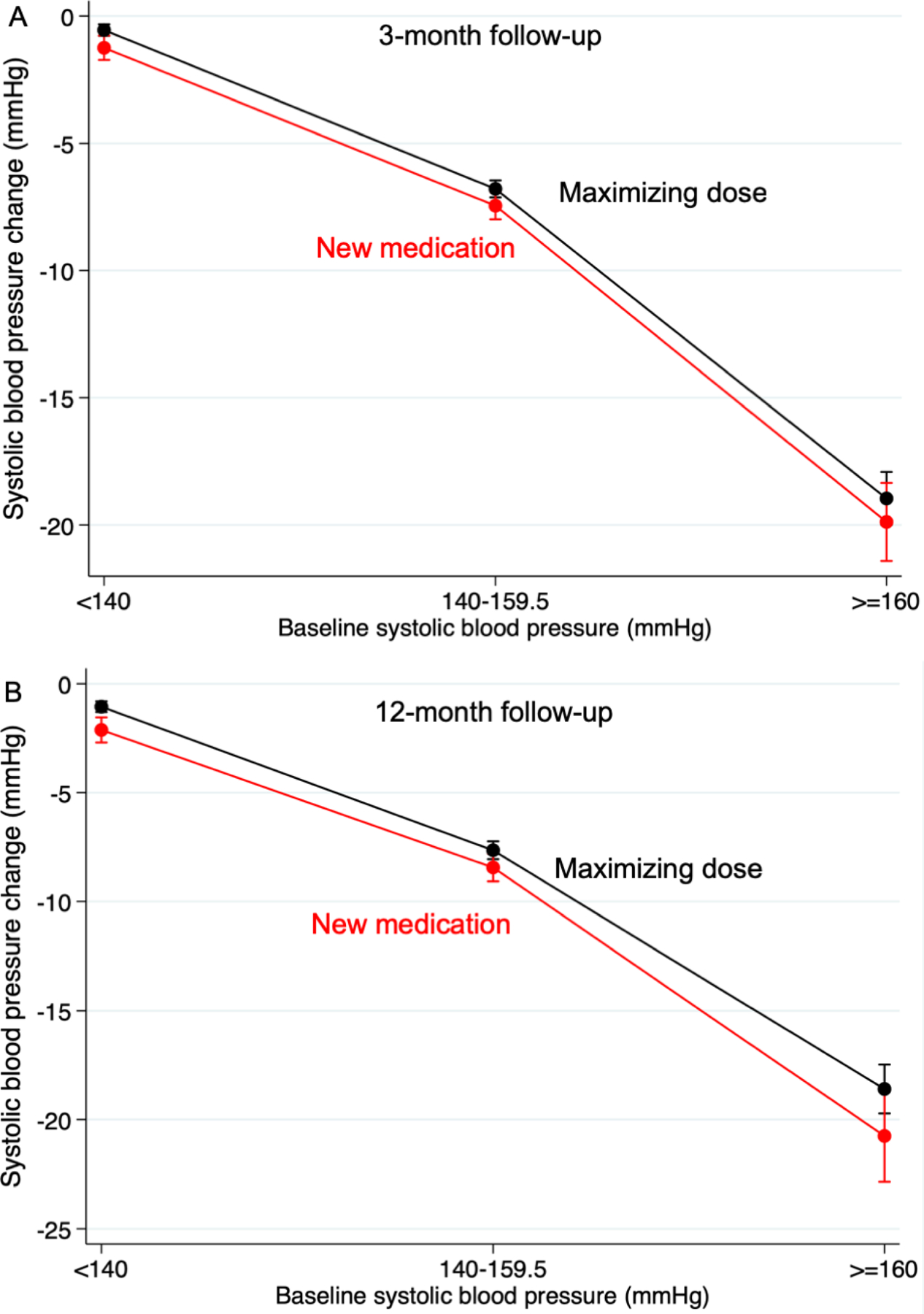
Results: Among 178 562 patients, 45 575 (25.5%) had intensification by adding a new medication and 132 987 (74.5%) by maximizing dose. Compared with maximizing dose, adding a new medication was associated with less intensification sustainability (average treatment effect, -15.2% [95% CI, -15.7% to -14.6%] at 3 months and -15.1% [CI, -15.6% to -14.5%] at 12 months) but a slightly larger reduction in mean SBP (-0.8 mm Hg [CI, -1.2 to -0.4 mm Hg] at 3 months and -1.1 mm Hg [CI, -1.6 to -0.6 mm Hg] at 12 months).
Limitation: Observational data; largely male population.
Conclusion: Adding a new antihypertensive medication was less frequent and was associated with less intensification sustainability but slightly larger reductions in SBP. Trials would provide the most definitive support for our findings.
Primary funding source: National Institute on Aging and Veterans Health Administration.
Figures
Comment in
-
How to Intensify Treatment in Older Patients With Hypertension: Is There a Single Answer?Ann Intern Med. 2021 Dec;174(12):1749-1750. doi: 10.7326/M21-3648. Epub 2021 Oct 5. Ann Intern Med. 2021. PMID: 34606314 No abstract available.
-
Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults.Ann Intern Med. 2022 Feb;175(2):W15-W16. doi: 10.7326/L21-0748. Ann Intern Med. 2022. PMID: 35157822 No abstract available.
-
Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults.Ann Intern Med. 2022 Feb;175(2):W15-W16. doi: 10.7326/L21-0749. Ann Intern Med. 2022. PMID: 35157823 No abstract available.
Similar articles
-
Hypertension treatment intensification among stroke survivors with uncontrolled blood pressure.Stroke. 2015 Feb;46(2):465-70. doi: 10.1161/STROKEAHA.114.007566. Epub 2014 Dec 30. Stroke. 2015. PMID: 25550374 Free PMC article.
-
Clinical outcomes of modifying hypertension treatment intensity in older adults treated to low blood pressure.J Am Geriatr Soc. 2021 Oct;69(10):2831-2841. doi: 10.1111/jgs.17295. Epub 2021 Jun 7. J Am Geriatr Soc. 2021. PMID: 34097300 Free PMC article.
-
Optimal systolic blood pressure target, time to intensification, and time to follow-up in treatment of hypertension: population based retrospective cohort study.BMJ. 2015 Feb 5;350:h158. doi: 10.1136/bmj.h158. BMJ. 2015. PMID: 25655523 Free PMC article.
-
Effect of Intensive Blood Pressure Lowering on Cardiovascular Outcomes: A Systematic Review Prepared for the 2020 U.S. Department of Veterans Affairs/U.S. Department of Defense Guidelines.Ann Intern Med. 2020 Dec 1;173(11):895-903. doi: 10.7326/M20-2037. Epub 2020 Sep 1. Ann Intern Med. 2020. PMID: 32866419
-
Updates in hypertension: new trials, targets and ways of measuring blood pressure.Curr Opin Nephrol Hypertens. 2022 May 1;31(3):258-264. doi: 10.1097/MNH.0000000000000791. Epub 2022 Mar 4. Curr Opin Nephrol Hypertens. 2022. PMID: 35249970 Free PMC article. Review.
Cited by
-
Reporting of Observational Studies Explicitly Aiming to Emulate Randomized Trials: A Systematic Review.JAMA Netw Open. 2023 Sep 5;6(9):e2336023. doi: 10.1001/jamanetworkopen.2023.36023. JAMA Netw Open. 2023. PMID: 37755828 Free PMC article.
-
Methodologies for the Emulation of Biomarker-Guided Trials Using Observational Data: A Systematic Review.J Pers Med. 2025 May 10;15(5):195. doi: 10.3390/jpm15050195. J Pers Med. 2025. PMID: 40423066 Free PMC article. Review.
-
Comparative Efficacy of Hypertension Management Strategies.Int J Angiol. 2024 Jul 4;33(4):297-302. doi: 10.1055/s-0044-1788068. eCollection 2024 Dec. Int J Angiol. 2024. PMID: 39502343 Free PMC article.
-
Use of sensitivity analyses to assess uncontrolled confounding from unmeasured variables in observational, active comparator pharmacoepidemiologic studies: a systematic review.Am J Epidemiol. 2025 Feb 5;194(2):524-535. doi: 10.1093/aje/kwae234. Am J Epidemiol. 2025. PMID: 39098826 Free PMC article.
-
Prognostic Nutritional Index as a Novel Predictor of Long-Term Prognosis in Patients with Coronary Artery Disease After Percutaneous Coronary Intervention.Clin Appl Thromb Hemost. 2022 Jan-Dec;28:10760296221103271. doi: 10.1177/10760296221103271. Clin Appl Thromb Hemost. 2022. PMID: 36001005 Free PMC article.
References
-
- Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. The New England journal of medicine. 2008;358(18):1887–98. - PubMed
-
- Wald DS, Law M, Morris JK, et al. Combination therapy versus monotherapy in reducing blood pressure: meta-analysis on 11,000 participants from 42 trials. The American journal of medicine. 2009;122(3):290–300. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical