

A Retrospective Case Series of Anesthetic Patients With Epiglottic Cysts
- PMID: 34606575
- PMCID: PMC8500314
- DOI: 10.2344/anpr-68-01-01
A Retrospective Case Series of Anesthetic Patients With Epiglottic Cysts
Abstract
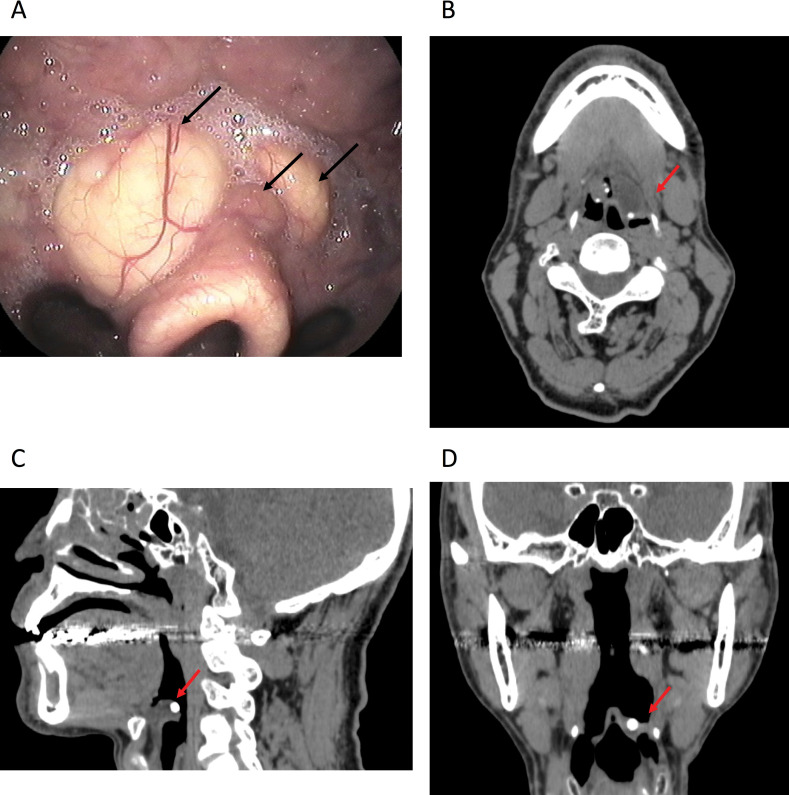
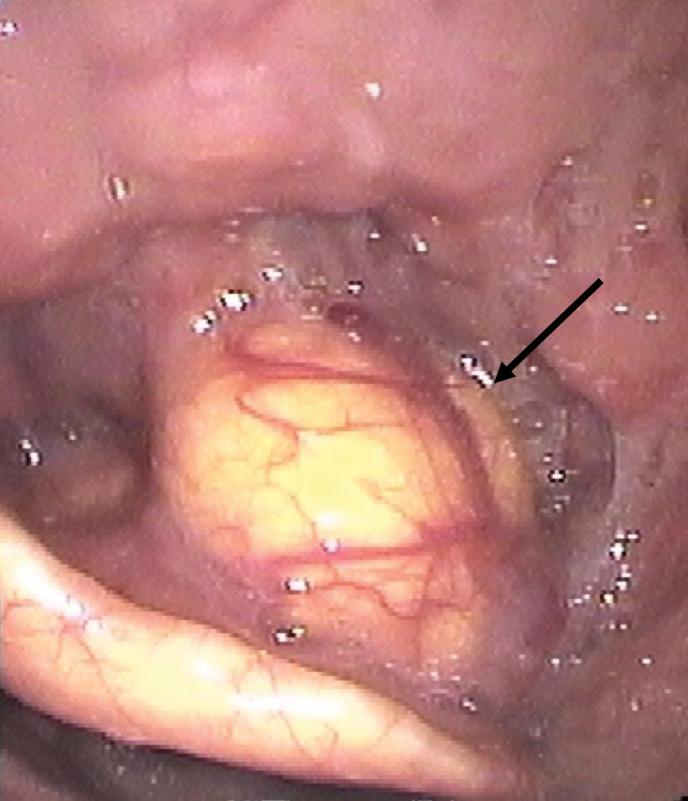
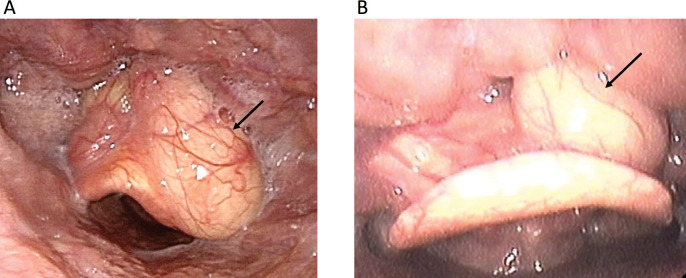
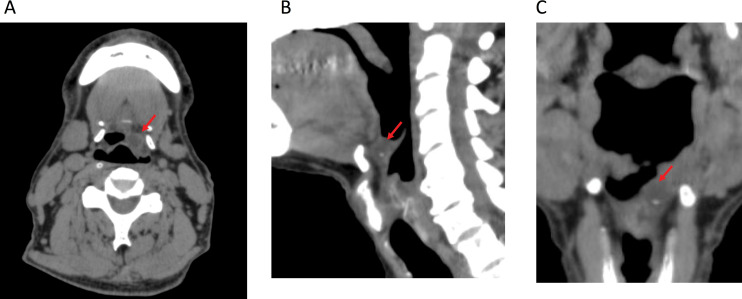
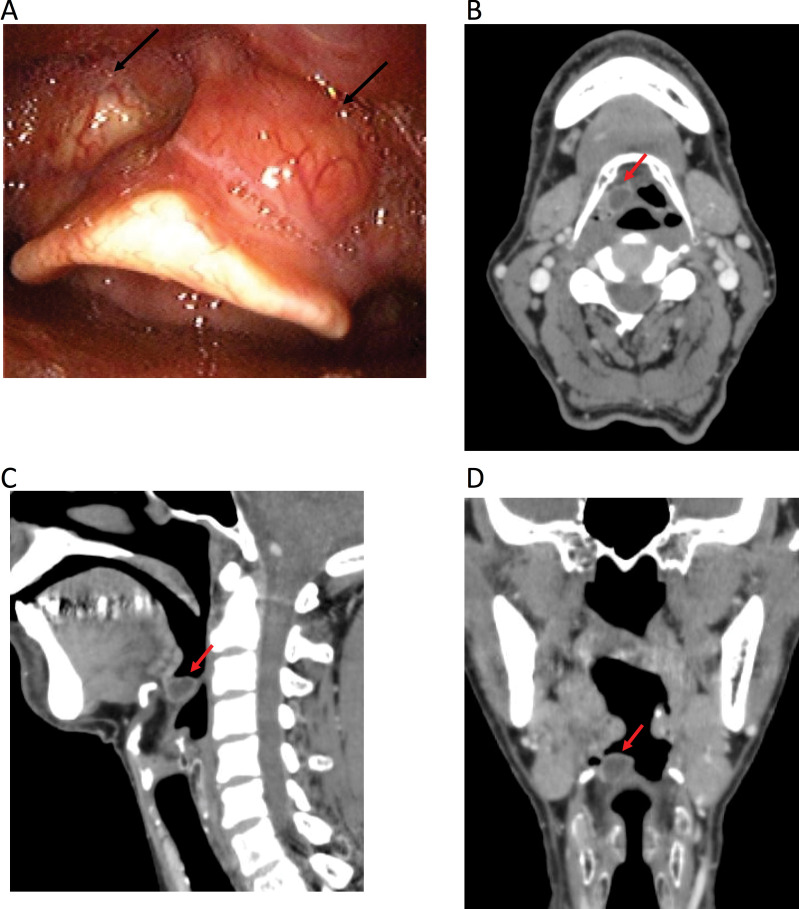
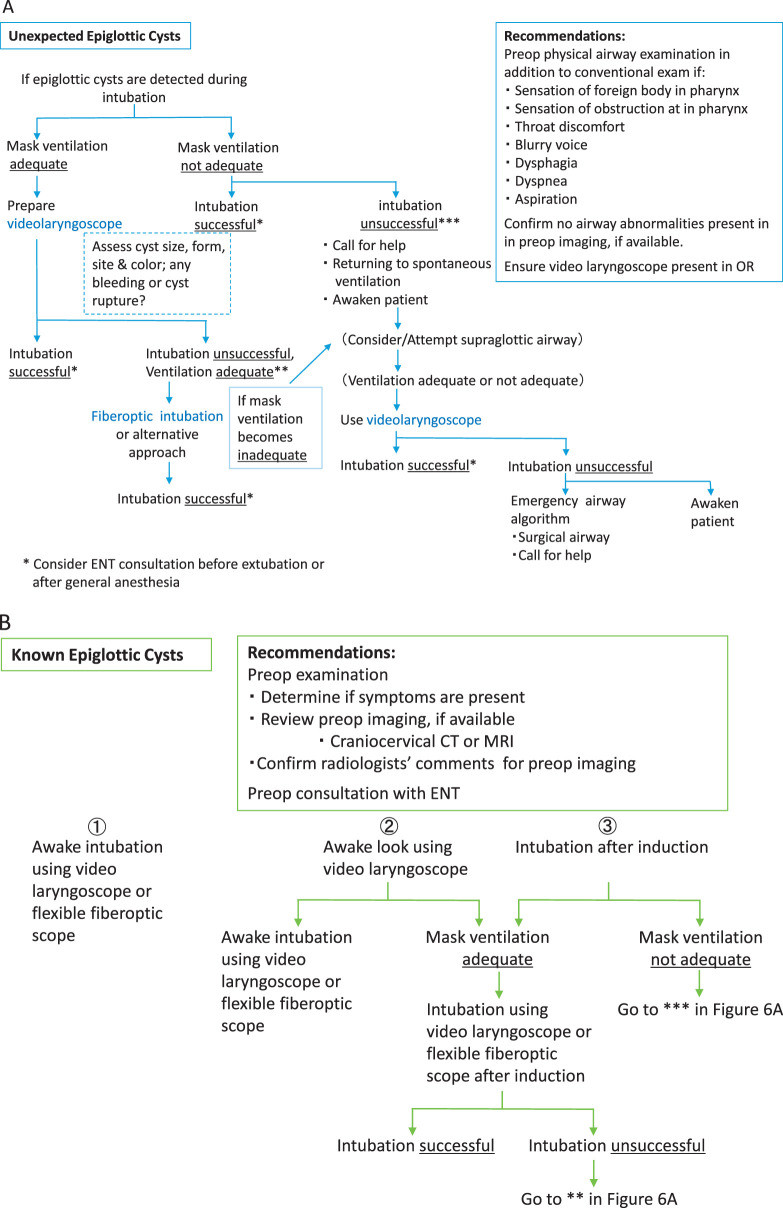
Previously undiagnosed or asymptomatic epiglottic cysts may be coincidentally detected during intubation. This retrospective case series identified undiagnosed epiglottic cysts that were discovered during intubation in 4 patients who underwent oral surgery under general anesthesia at our hospital during a 6-year period. Including 2 additional cases, 1 previously diagnosed and 1 detected during preoperative imaging, epiglottic cysts were observed in 6 of 1112 cases (0.54%) total. Among the undiagnosed epiglottic cyst cases, mild dyspnea on effort or snoring was reported in 2 patients, but all others were asymptomatic. Upon discovering previously undiagnosed epiglottic cysts during intubation, it is essential to proceed cautiously, remain alert for potential airway management difficulties, and avoid injuring or rupturing the cysts. In addition, any available preoperative imaging should be reviewed as information pertinent to the airway and any abnormalities may be useful. This report discusses the anesthetic care of 6 patients with epiglottic cysts that were previously known or initially discovered during intubation.
Keywords: Airway management; Epiglottic cyst; General anesthesia; Laryngoscopy.
© 2021 by the American Dental Society of Anesthesiology.
Figures
References
-
- Padfield A. Epiglottic cysts. A case report and review. Anaesthesia. 1972;27:84–88. - PubMed
-
- Asherson N. Large cysts of the epiglottis: a classification and case records. J Laryngol Otol. 1957;71:730–743. - PubMed
-
- Vorobeichik L, Hare GM, Zirkle M, Garavagia MM. Airway management of incidental vallecular cysts in adults. A A Case Rep. 2015;5:223–227. - PubMed
-
- Marseglia L, D'Angelo G, Impellizzeri P, et al. Neonatal stridor and laryngeal cyst: which comes first? Pediatric Int. 2017;59:115–117. - PubMed
-
- Gilbey P, Amirav I, Luder A. Vallecular cyst: rare cause of failure to thrive without respiratory distress in an infant. J Pediatr. 2011;159:869. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
