

TSST-1+Staphylococcus aureus in Bullous Pemphigoid
- PMID: 34606884
- PMCID: PMC9215375
- DOI: 10.1016/j.jid.2021.08.438
TSST-1+Staphylococcus aureus in Bullous Pemphigoid
Abstract
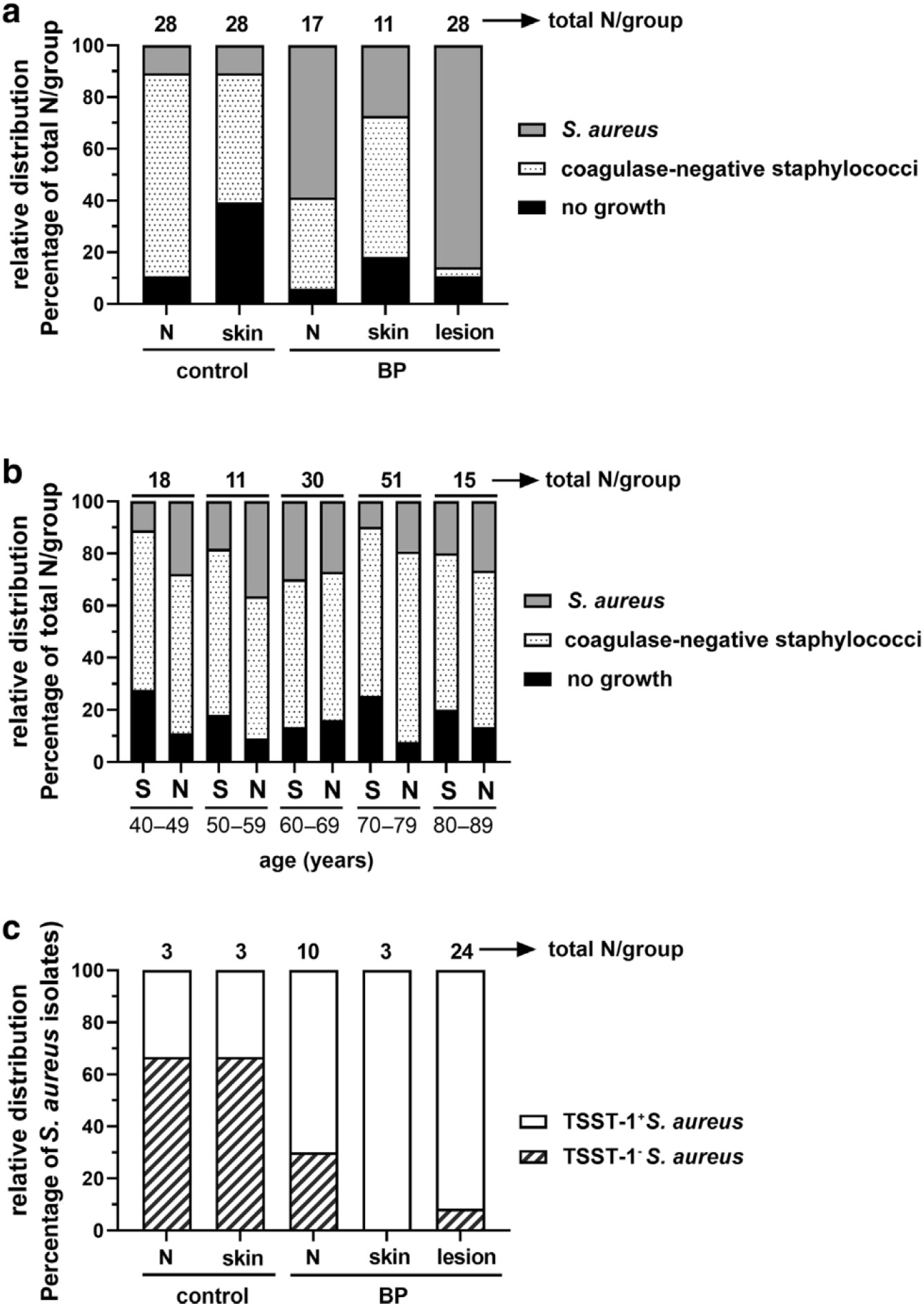
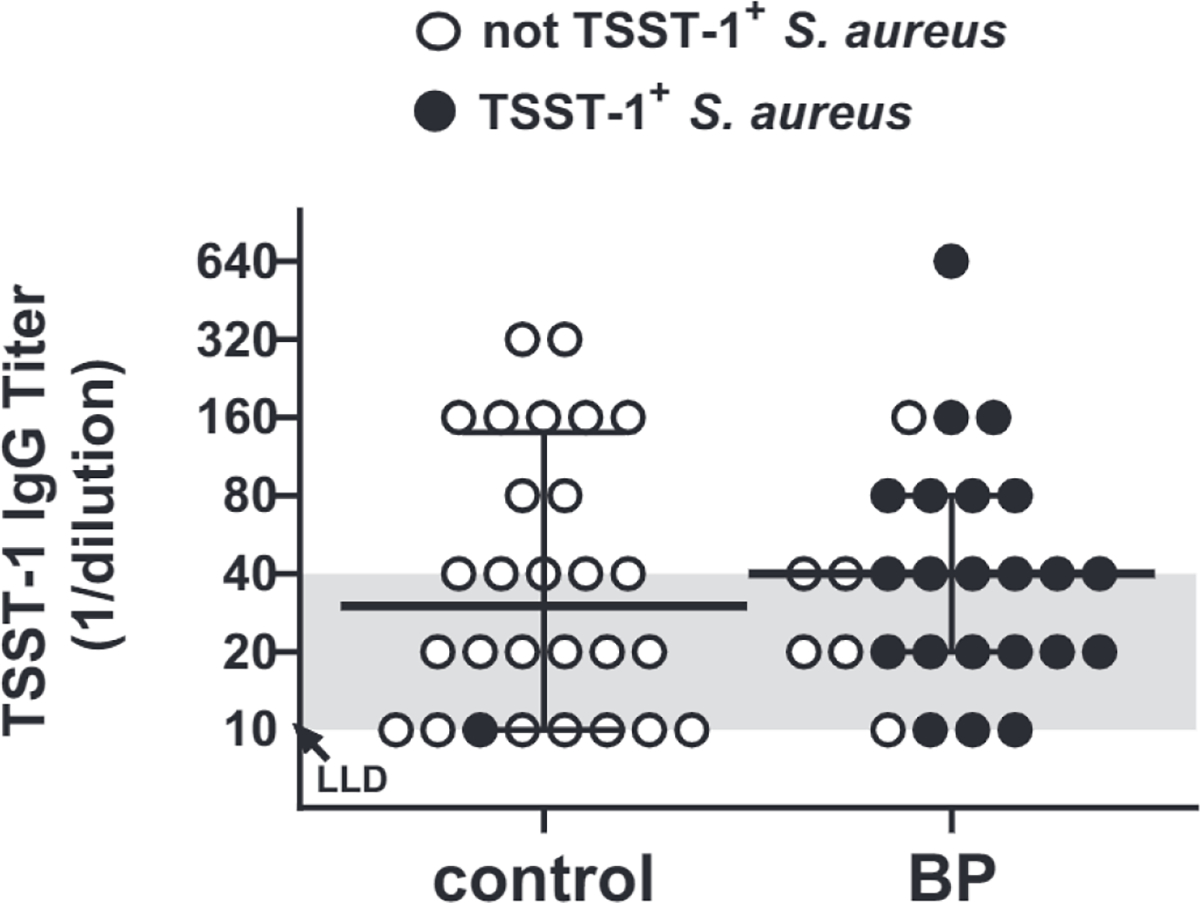
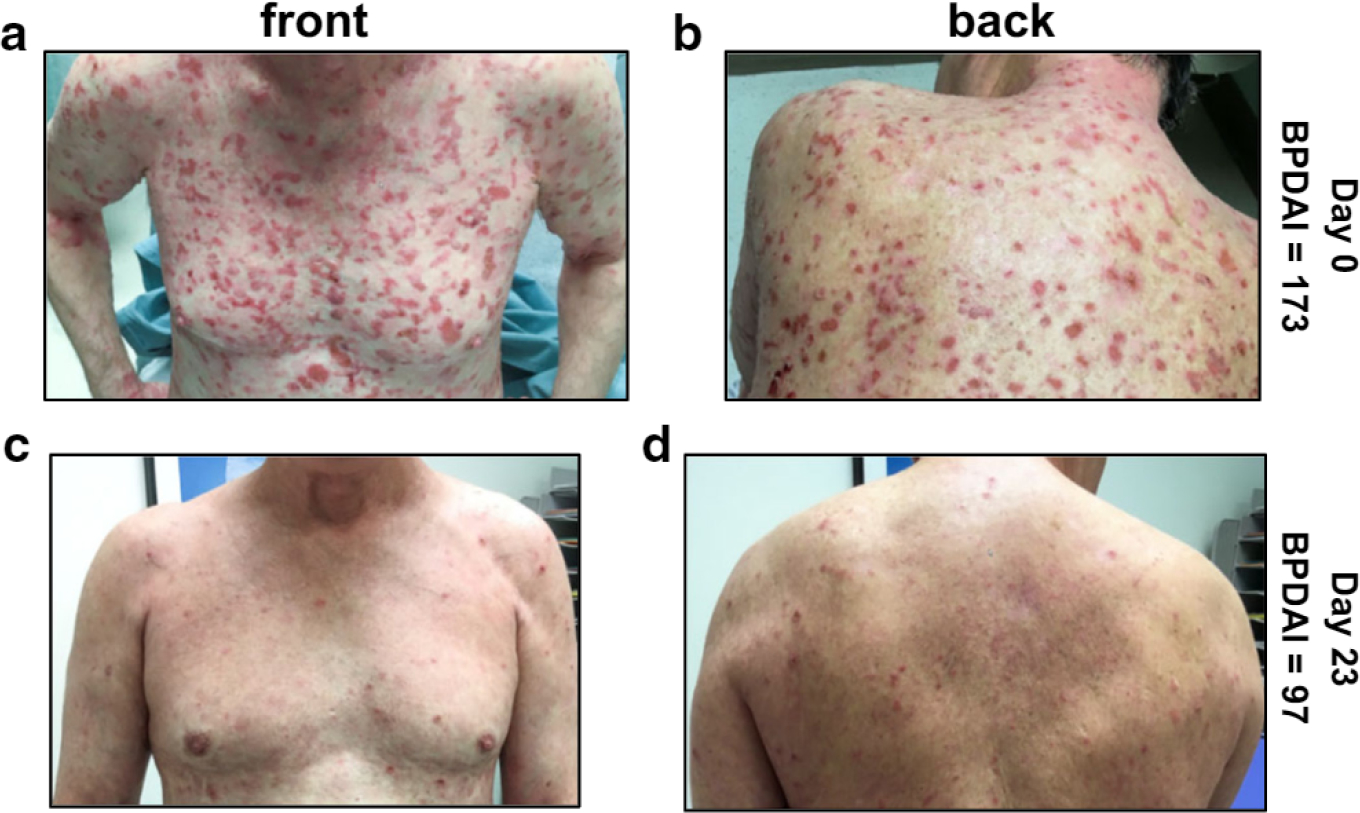
A potential role of Staphylococcus aureus in bullous pemphigoid was explored by examining the colonization rate in patients with new-onset disease compared with that in age- and sex-matched controls. S. aureus colonization was observed in 85% of bullous pemphigoid lesions, 3-6-fold higher than the nares or unaffected skin from the same patients (P ≤ 0.003) and 6-fold higher than the nares or skin of controls (P ≤ 0.0015). Furthermore, 96% of the lesional isolates produced the toxic shock syndrome toxin-1 superantigen, and most of these additionally exhibited homogeneous expression of the enterotoxin gene cluster toxins. Toxic shock syndrome toxin-1‒neutralizing antibodies were not protective against colonization. However, S. aureus colonization was not observed in patients who had recently received antibiotics, and the addition of antibiotics with staphylococcal coverage eliminated S. aureus and resulted in clinical improvement. This study shows that toxic shock syndrome toxin-1‒positive S. aureus is prevalent in bullous pemphigoid lesions and suggests that early implementation of antibiotics may be of benefit. Furthermore, our results suggest that S. aureus colonization could provide a source of infection in patients with bullous pemphigoid, particularly in the setting of high-dose immunosuppression.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
CONFLICT OF INTEREST
All authors state no conflict of interest.
Figures
References
-
- Ameglio F, D’Auria L, Bonifati C, Ferraro C, Mastroianni A, Giacalone B. Cytokine pattern in blister fluid and serum of patients with bullous pemphigoid: relationships with disease intensity. Br J Dermatol 1998;138:611–4. - PubMed
-
- Blomster-Hautamaa DA, Schlievert PM. Preparation of toxic shock syndrome toxin-1. Methods Enzymol 1988;165:37–43. - PubMed
-
- Chen C, Zhang M, Chen H, Fang J. Subtherapeutic linezolid concentration in a patient with bullous pemphigoid complicated by methicillin-resistant Staphylococcus aureus infection: a case study. Ther Drug Monit 2020;42:515–7. - PubMed
-
- D’Auria L, Cordiali Fei P, Ameglio F. Cytokines and bullous pemphigoid. Eur Cytokine Netw 1999;10:123–34. - PubMed
-
- Diaz LA, Ratrie H, Saunders W, Futamura S, Squiquera F, Anhalt J, et al. Isolation of a human epidermal cDNA corresponding to the 180-kD autoantigen recognized by bullous pemphigoid and herpes gestationis sera Immunolocalization of this protein to the hemidesmosome. J Clin Investig 1990;86:1088–94. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
