

First-line nivolumab plus ipilimumab with two cycles of chemotherapy versus chemotherapy alone (four cycles) in advanced non-small-cell lung cancer: CheckMate 9LA 2-year update
- PMID: 34607285
- PMCID: PMC8493593
- DOI: 10.1016/j.esmoop.2021.100273
First-line nivolumab plus ipilimumab with two cycles of chemotherapy versus chemotherapy alone (four cycles) in advanced non-small-cell lung cancer: CheckMate 9LA 2-year update
Erratum in
-
Corrigendum to 'First-line nivolumab plus ipilimumab with 2 cycles of chemotherapy versus chemotherapy alone (4 cycles) in advanced non-small cell lung cancer: CheckMate 9LA 2-year update': [ESMO Open Volume 6, Issue 5, October 2021, 100273].ESMO Open. 2021 Dec;6(6):100345. doi: 10.1016/j.esmoop.2021.100345. Epub 2021 Dec 2. ESMO Open. 2021. PMID: 34864501 Free PMC article. No abstract available.
Abstract
Background: To further characterize survival benefit with first-line nivolumab plus ipilimumab with two cycles of chemotherapy versus chemotherapy alone, we report updated data from the phase III CheckMate 9LA trial with a 2-year minimum follow-up.
Patients and methods: Adult patients were treatment naïve, with stage IV/recurrent non-small-cell lung cancer, no known sensitizing EGFR/ALK alterations, and an Eastern Cooperative Oncology Group performance status ≤1. Patients were randomized 1 : 1 to nivolumab 360 mg every 3 weeks plus ipilimumab 1 mg/kg every 6 weeks with two cycles of chemotherapy, or four cycles of chemotherapy. Updated efficacy and safety outcomes are reported, along with progression-free survival (PFS) after next line of treatment (PFS2), treatment-related adverse events (TRAEs) by treatment cycle, and efficacy outcomes in patients who discontinued all treatment components in the experimental arm due to TRAEs.
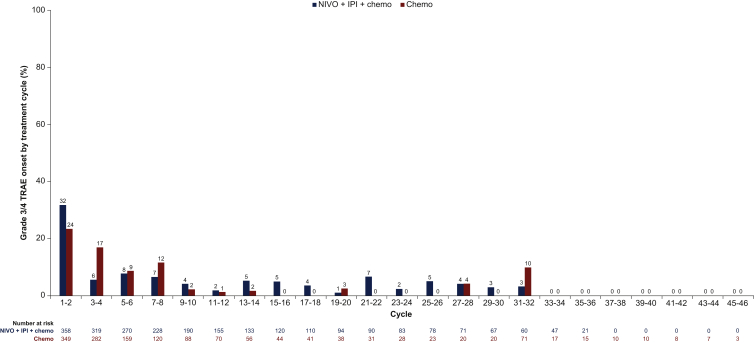
Results: With a median follow-up of 30.7 months, nivolumab plus ipilimumab with chemotherapy continued to prolong overall survival (OS) versus chemotherapy. Median OS was 15.8 versus 11.0 months [hazard ratio 0.72 (95% confidence interval 0.61-0.86)]; 2-year OS rate was 38% versus 26%. Two-year PFS rate was 20% versus 8%. ORR was 38% versus 25%, respectively; 34% versus 12% of all responses were ongoing at 2 years. Median PFS2 was 13.9 versus 8.7 months. Improved efficacy outcomes in the experimental versus control arm were observed across most subgroups, including by programmed death-ligand 1 and histology. No new safety signals were observed; onset of grade 3/4 TRAEs was mostly observed during the first two treatment cycles in the experimental arm. In patients who discontinued all components of nivolumab plus ipilimumab with chemotherapy treatment due to TRAEs (n = 61) median OS was 27.5 months; 56% of responders had an ongoing response ≥1 year after discontinuation.
Conclusions: With a 2-year minimum follow-up, nivolumab plus ipilimumab with two cycles of chemotherapy provided durable efficacy benefits over chemotherapy with a manageable safety profile and remains an efficacious first-line treatment of advanced non-small-cell lung cancer.
Keywords: NSCLC; dual immunotherapy; first-line; ipilimumab; nivolumab.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure MR reports advisory/consulting fees from AbbVie, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Mirati Therapeutics, MSD Oncology, Novartis, Pfizer, Roche/Genentech, and Samsung Bioepis; speaker fees from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Merck Serono, Mirati Therapeutics, MSD Oncology, Novartis, Pfizer, and Roche/Genentech. TEC reports advisory/consulting fees and travel, accommodation, and expenses from Amgen, Astellas, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Ipsen, Janssen, Merck Sharp & Dohme (MSD), Novartis/GlaxoSmithKline, Pfizer, Roche, Sanofi, and Servier. MS reports research funding from AbbVie, Amgen, Astellas Pharma, AstraZeneca, Bristol Myers Squibb, Clovis, Eli Lilly, Gilead Sciences, GlaxoSmithKline, MSD, Novartis, Pfizer/EMD Serono, Regeneron, Roche, and Tesaro; travel, accommodation, and expenses from Bristol Myers Squibb. BZ reports research funding from Amgen, AstraZeneca, Bristol Myers Squibb, GlaxoSmithKline, Janssen-Cilag, MSD, and Roche. JB reports advisory/consulting fees and honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, MSD, Roche, and Servier; travel, accommodation, and expenses from AstraZeneca and Roche. EF reports advisory fees from AbbVie, Amgen, AstraZeneca, Bayer, BeiGene, Blue Print Medicines, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen, Medical Trends, Merck KGaA, MSD, Novartis, Peptomyc, Pfizer, Puma Biotechnology, Regeneron, Roche, Sanofi Genzyme, Syneos Health, Takeda; independent board member of Grifols; research funding from Grant for Oncology Innovation and Fundación Merck Salud; speaker fees from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Medscape, MSD, Novartis, PeerVoice, Pfizer, Prime Oncology, Roche, Springer, Takeda, Touch Medical, and CME Outfitters. OJV reports advisory/consulting fees from Boehringer Ingelheim, Bristol Myers Squibb, Lilly, MSD, Roche/Genetech, and Takeda; honoraria from AstraZeneca/MedImmune, Bristol Myers Squibb, MSD Oncology, and Roche/Genentech; research funding from AstraZeneca Spain; speaker fees from Roche/Genentech; travel, accommodation, and expenses from Boehringer Ingelheim, Bristol Myers Squibb, MSD, and Roche/Genentech. AA reports advisory/consulting fees from Boehringer Ingelheim Pharmaceuticals Inc and Roche; expert testimony fees for AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Pfizer, Roche, and Sanofi; speaker fees from Bristol Myers Squibb, Novartis, and Sandoz; travel, accommodation, and expenses from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Pfizer, Roche, and Sanofi. HS reports research funding from AstraZeneca, Bristol Myers Squibb, Chugai Pharma, Merck KGaA, MSD K.K, Ono Pharmaceutical, and Taiho Pharmaceutical; speaker fees from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb Japan, Chugai Pharma, MSD K.K, Ono Pharmaceutical, and Taiho Pharmaceutical. FR reports consulting and speaker fees from Novartis; travel, accommodation, and expenses from Roche. PJS reports non-financial support from AstraZeneca, Bristol Myers Squibb, MSD, and Roche; personal fees from AstraZeneca, Bristol Myers Squibb, Novartis, and Roche; research funding from AstraZeneca, Bristol Myers Squibb, Novartis, MSD, and Roche. CM reports advisory and speaker fees from AstraZeneca, Bristol Myers Squibb, and MSD. MP reports advisory fees from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, MSD, Novartis, Pfizer, Roche, and Takeda; research funding from AstraZeneca, Boehringer Ingelheim, Chugai, Roche, and Takeda; speaker fees from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Chugai, Eli Lilly, MSD, Pfizer, Roche, and Takeda; travel support from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Chugai, Eli Lilly, MSD, Pfizer, Roche, and Takeda. AS reports expert testimony fees from AstraZeneca/MedImmune, Bristol Myers Squibb, MSD Oncology, and Roche; research funding from Bristol Myers Squibb; speaker fees from AstraZeneca/MedImmune; travel, accommodation, and expenses from AstraZeneca/MedImmune, Bristol Myers Squibb, MSD Oncology, and Roche. SL reports advisory/consulting fees from AstraZeneca, Boehringer Ingelheim, Hutchison MediPharma, Roche, and Simcere; research funding from AstraZeneca, Bristol Myers Squibb, Hutchison MediPharma, Heng Rui, and Roche; speaker fees from AstraZeneca, Hanseng, and Roche. LPA reports honoraria from Amgen, AstraZeneca, Bayer, Blueprint Medicines, Bristol Myers Squibb, Celgene, Ipsen, Eli Lilly, Merck Serono, Mirati Therapeutics, MSD, Novartis, Pfizer, PharmaMar, Roche/Genentech, Sanofi, Servier, and Takeda; leadership fees from Genomica and ALTUM Sequencing; research funding from AstraZeneca, Bristol Myers Squibb, Kura Oncology, PharmaMar, and MSD; speaker fees from Bristol Myers Squibb, Eli Lilly, Merck Serono, MSD Oncology, Pfizer, Roche/Genentech; travel, accommodation, and expenses from AstraZeneca, Bristol Myers Squibb, MSD, Pfizer, Roche, and Takeda. DPC reports advisory/consulting fees from AbbVie, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Bristol Myers Squibb Japan, Curio Science, Daiichi Sankyo, Eli Lilly, EMD Serono, Flame Biosciences, G1 Therapeutics (Intellisphere), Geneplus, GlaxoSmithKline, Gloria Biosciences, Incyte, Inivata, Inovio Pharmaceutical, Janssen, Johnson & Johnson, Kyowa Hakko Kirin, Loxo, Merck, Merck KGaA, MSD, Novartis, Novocure, Oncocyte, OncoHost, Pfizer, Piper Sandler, Roche/Genentech, Sanofi, and Takeda; employment with James Cancer Center; honoraria from AstraZeneca and Nexus Pharmaceutical; research funding from Bristol Myers Squibb. AM is an employee of and has stock ownership in Bristol Myers Squibb. SM is an employee of and has stock ownership in Bristol Myers Squibb; was employed as a contractor by Sanofi (Rangam Consultants Inc); reports travel, accommodation, and expenses from Bristol Myers Squibb. XZ is an employee of Bristol Myers Squibb. PT is an employee of and has stock ownership in Bristol Myers Squibb. TJ reports advisory/consulting fees from AstraZeneca, AstraZeneca/MedImmune, Boehringer Ingelheim, Bristol Myers Squibb, Ignyta, Merck KGaA, MSD Oncology, Novartis, Pfizer, and Roche/Genentech; honoraria from AstraZeneca/MedImmune, Bristol Myers Squibb, MSD Oncology, and Roche/Genentech; travel, accommodation, and expenses from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, MSD, and Roche. All other authors have declared no conflicts of interest.
Figures





References
-
- Hellmann M.D., Paz-Ares L., Bernabe Caro R. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N Engl J Med. 2019;381:2020–2031. - PubMed
-
- Reck M., Rodriguez-Abreu D., Robinson A.G. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. - PubMed
-
- Mok T.S.K., Wu Y.L., Kudaba I. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819–1830. - PubMed
-
- Paz-Ares L., Luft A., Vicente D. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040–2051. - PubMed
-
- West H., McCleod M., Hussein M. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20(7):924–937. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
