

A retrospective medical chart review of clinical outcomes in children and adolescents with attention-deficit/hyperactivity disorder treated with guanfacine extended-release in routine Canadian clinical practice
- PMID: 34607580
- PMCID: PMC8491395
- DOI: 10.1186/s13034-021-00402-5
A retrospective medical chart review of clinical outcomes in children and adolescents with attention-deficit/hyperactivity disorder treated with guanfacine extended-release in routine Canadian clinical practice
Abstract
Objective: This study evaluated clinical outcomes in children and adolescents with attention-deficit/hyperactivity disorder (ADHD) treated with the α2-adrenoceptor agonist guanfacine extended-release (GXR) in routine Canadian clinical practice.
Methods: This retrospective chart review focused on patients with ADHD aged 6-17 years initiating treatment with GXR as monotherapy or adjunctive therapy. Patients were followed for up to 12 months after GXR initiation and, if they had received prior ADHD pharmacotherapy, for 12 months before GXR initiation. The primary outcome was change in ADHD symptoms and functionality based on physician assessments, classified as improvement, no change, or worsening relative to the time of GXR initiation. Treatment-emergent adverse events (TEAEs) were evaluated. Clinical outcomes were also analyzed post hoc according to whether GXR treatment was received as monotherapy or adjunctive therapy, and by select psychiatric comorbidities. Exploratory analyses were conducted in patients who had received prior ADHD pharmacotherapy to evaluate clinical outcomes after initiating GXR.
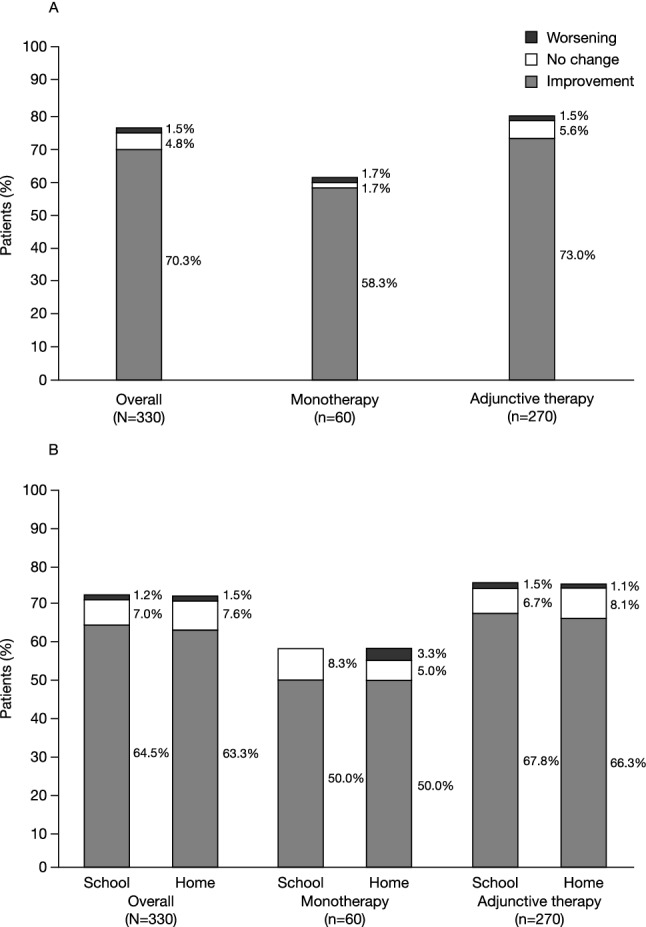
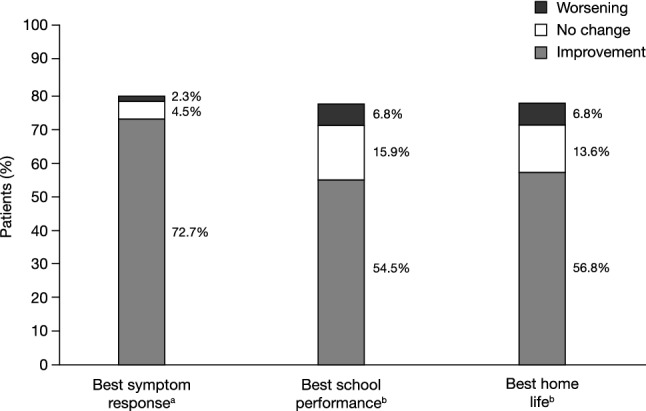
Results: Improvements in ADHD symptoms were reported for 232/330 (70.3%) patients. Functional improvements in school performance and home life were reported for 213/330 (64.5%) and 209/330 (63.3%) patients, respectively. The most frequent TEAEs (≥ 5%) were somnolence, headache, insomnia, presyncope, and decreased appetite. Improvements in ADHD symptoms were observed when GXR was received as either monotherapy (35/60 [58.3%]) or adjunctive therapy (197/270 [73.0%]). Improvements in ADHD symptoms and functionality were observed in the majority of patients with select psychiatric comorbidities. Among patients who had experienced worsening of symptoms with prior ADHD pharmacotherapy, 44/54 (81.5%) experienced symptom improvement, 33/44 (75.0%) who had previously experienced worsening of school performance improved, and 34/48 (70.8%) who had previously experienced worsening of home life improved.
Conclusion: In Canadian routine clinical practice, most children and adolescents with ADHD treated with GXR experienced improvements in ADHD symptoms and in functionality both at school and at home.
Keywords: ADHD; ADHD symptoms; Chart review; Guanfacine extended-release; Non-stimulant.
© 2021. The Author(s).
Conflict of interest statement
JvS has received compensation for serving as a consultant and speaker for Janssen, Purdue Pharma, and Takeda Canada Inc. JvS has also received educational grants from Janssen, Purdue Pharma, and Takeda Canada Inc., and research grants from Emalex, Janssen, Nuvelution, Purdue Pharma, Takeda Canada Inc., Biohaven and Teva. JvS has also participated in advisory boards and speaker bureaus for Janssen, Purdue Pharma, and Takeda Canada Inc. JvS owns stocks in Johnson & Johnson. SKG is an employee of Takeda Canada Inc. SKG owns stock/stock options in Takeda. CJR was an employee of Shire Pharma Canada ULC (now Takeda Canada Inc.) at the time of the study. CJR is currently an employee of Medison Canada. KH has received research grants and speaking honoraria from Takeda Canada Inc., and has acted on advisory boards and speaker bureaus for Sunovion, Janssen, Purdue, and Takeda Canada Inc.
Figures
Similar articles
-
Efficacy and safety of extended-release guanfacine hydrochloride in children and adolescents with attention-deficit/hyperactivity disorder: a randomized, controlled, phase III trial.Eur Neuropsychopharmacol. 2014 Dec;24(12):1861-72. doi: 10.1016/j.euroneuro.2014.09.014. Epub 2014 Oct 23. Eur Neuropsychopharmacol. 2014. PMID: 25453486 Clinical Trial.
-
Is adjunctive pharmacotherapy in attention-deficit/hyperactivity disorder cost-effective in Canada: a cost-effectiveness assessment of guanfacine extended-release as an adjunctive therapy to a long-acting stimulant for the treatment of ADHD.BMC Psychiatry. 2016 Jan 16;16:11. doi: 10.1186/s12888-016-0708-x. BMC Psychiatry. 2016. PMID: 26774811 Free PMC article.
-
A Randomized, Placebo-Controlled Trial of Guanfacine Extended Release in Adolescents With Attention-Deficit/Hyperactivity Disorder.J Am Acad Child Adolesc Psychiatry. 2015 Nov;54(11):916-25.e2. doi: 10.1016/j.jaac.2015.08.016. Epub 2015 Sep 15. J Am Acad Child Adolesc Psychiatry. 2015. PMID: 26506582 Clinical Trial.
-
Guanfacine extended release: a novel treatment for attention-deficit/hyperactivity disorder in children and adolescents.Clin Ther. 2013 Nov;35(11):1778-93. doi: 10.1016/j.clinthera.2013.09.005. Epub 2013 Oct 16. Clin Ther. 2013. PMID: 24139092 Review.
-
Guanfacine extended release as adjunctive therapy to psychostimulants in children and adolescents with attention-deficit/hyperactivity disorder.Adv Ther. 2012 May;29(5):385-400. doi: 10.1007/s12325-012-0020-1. Epub 2012 May 18. Adv Ther. 2012. PMID: 22610723 Review.
Cited by
-
The Biology and Biochemistry of Kynurenic Acid, a Potential Nutraceutical with Multiple Biological Effects.Int J Mol Sci. 2024 Aug 21;25(16):9082. doi: 10.3390/ijms25169082. Int J Mol Sci. 2024. PMID: 39201768 Free PMC article. Review.
References
-
- Visser SN, Danielson ML, Bitsko RH, Holbrook JR, Kogan MD, Ghandour RM, et al. Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003–2011. J Am Acad Child Adolesc Psychiatry. 2014;53(1):34–46.e32. doi: 10.1016/j.jaac.2013.09.001. - DOI - PMC - PubMed
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders (DSM-5) 5. Arlington: American Psychiatric Publishing; 2013.
LinkOut - more resources
Full Text Sources
