

Prediction of operative mortality for patients undergoing cardiac surgical procedures without established risk scores
- PMID: 34607725
- PMCID: PMC8918430
- DOI: 10.1016/j.jtcvs.2021.09.010
Prediction of operative mortality for patients undergoing cardiac surgical procedures without established risk scores
Abstract
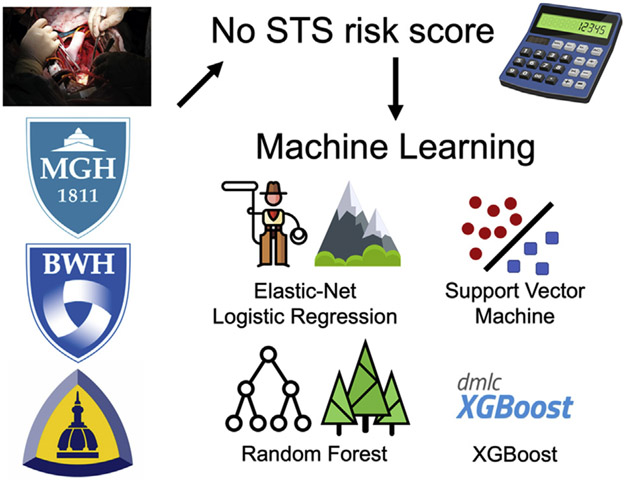
Objective: Current cardiac surgery risk models do not address a substantial fraction of procedures. We sought to create models to predict the risk of operative mortality for an expanded set of cases.
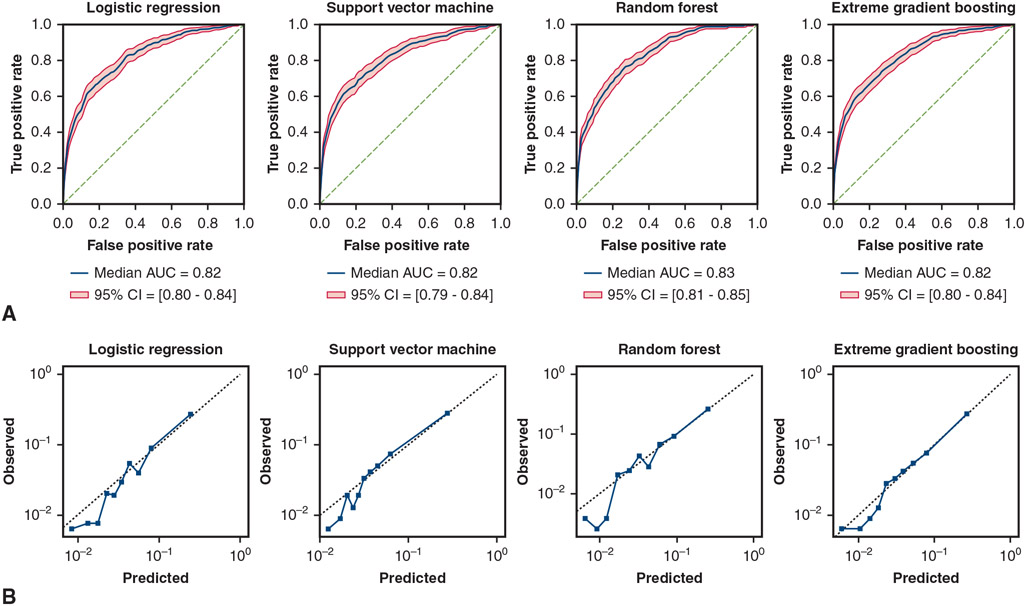
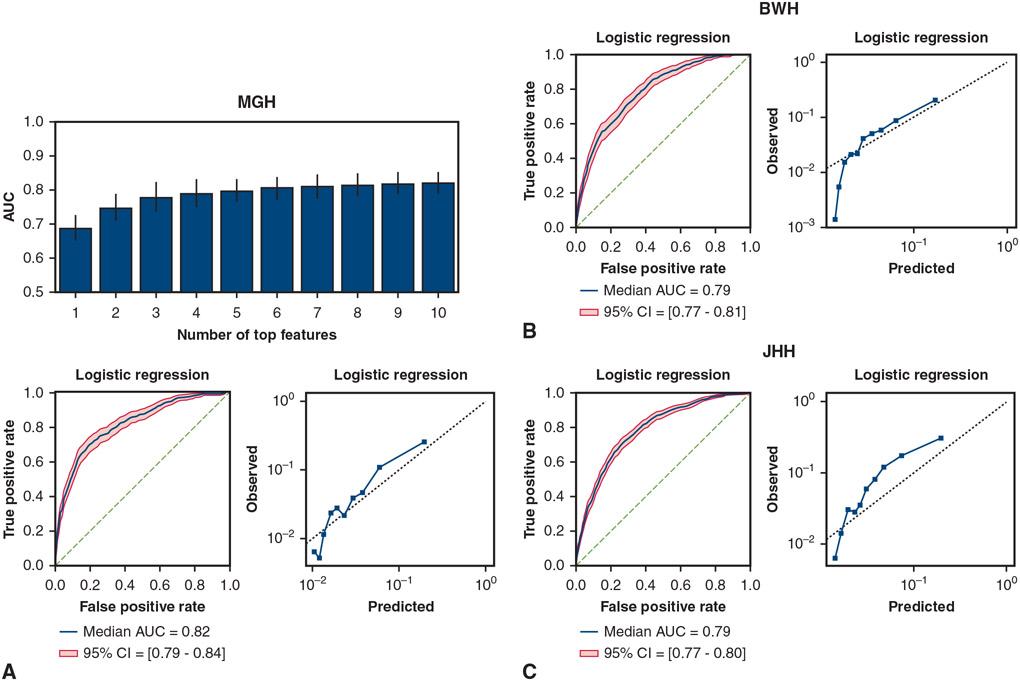
Methods: Four supervised machine learning models were trained using preoperative variables present in the Society of Thoracic Surgeons (STS) data set of the Massachusetts General Hospital to predict and classify operative mortality in procedures without STS risk scores. A total of 424 (5.5%) mortality events occurred out of 7745 cases. Models included logistic regression with elastic net regularization (LogReg), support vector machine, random forest (RF), and extreme gradient boosted trees (XGBoost). Model discrimination was assessed via area under the receiver operating characteristic curve (AUC), and calibration was assessed via calibration slope and expected-to-observed event ratio. External validation was performed using STS data sets from Brigham and Women's Hospital (BWH) and the Johns Hopkins Hospital (JHH).
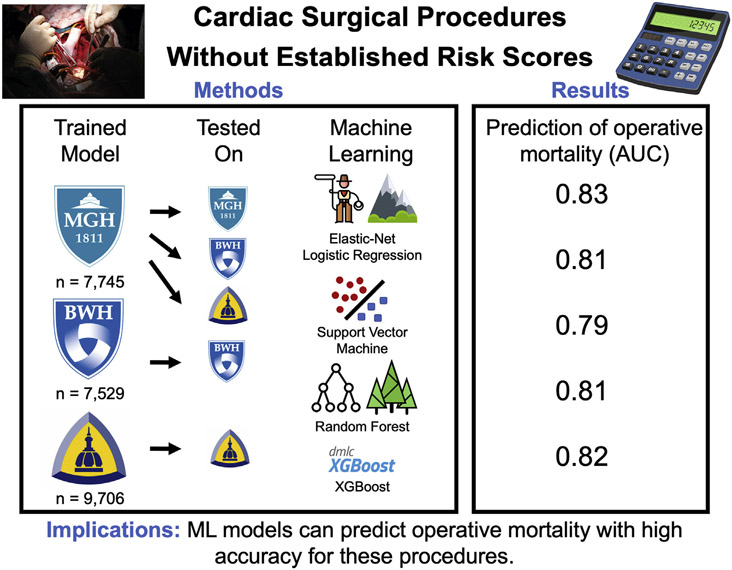
Results: Models performed comparably with the highest mean AUC of 0.83 (RF) and expected-to-observed event ratio of 1.00. On external validation, the AUC was 0.81 in BWH (RF) and 0.79 in JHH (LogReg/RF). Models trained and applied on the same institution's data achieved AUCs of 0.81 (BWH: LogReg/RF/XGBoost) and 0.82 (JHH: LogReg/RF/XGBoost).
Conclusions: Machine learning models trained on preoperative patient data can predict operative mortality at a high level of accuracy for cardiac surgical procedures without established risk scores. Such procedures comprise 23% of all cardiac surgical procedures nationwide. This work also highlights the value of using local institutional data to train new prediction models that account for institution-specific practices.
Keywords: cardiac surgery; machine learning; operative mortality; risk prediction.
Copyright © 2021 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement
The authors reported no conflicts of interest.
The
Figures
Comment in
-
Commentary: Improving the clarity of the crystal ball in cardiac surgery.J Thorac Cardiovasc Surg. 2023 Apr;165(4):1460-1461. doi: 10.1016/j.jtcvs.2021.09.045. Epub 2021 Oct 1. J Thorac Cardiovasc Surg. 2023. PMID: 34742537 No abstract available.
Similar articles
-
Prediction of the development of acute kidney injury following cardiac surgery by machine learning.Crit Care. 2020 Jul 31;24(1):478. doi: 10.1186/s13054-020-03179-9. Crit Care. 2020. PMID: 32736589 Free PMC article.
-
Predictive Utility of a Machine Learning Algorithm in Estimating Mortality Risk in Cardiac Surgery.Ann Thorac Surg. 2020 Jun;109(6):1811-1819. doi: 10.1016/j.athoracsur.2019.09.049. Epub 2019 Nov 7. Ann Thorac Surg. 2020. PMID: 31706872
-
Comparison of machine learning techniques in prediction of mortality following cardiac surgery: analysis of over 220 000 patients from a large national database.Eur J Cardiothorac Surg. 2023 Jun 1;63(6):ezad183. doi: 10.1093/ejcts/ezad183. Eur J Cardiothorac Surg. 2023. PMID: 37154705 Free PMC article.
-
Evidence-Based Determination of Cut-Off Points for Increased Cardiac-Surgery Mortality Risk With EuroSCORE II and STS: The Best-Performing Risk Scoring Models in a Single-Centre Australian Population.Heart Lung Circ. 2022 Apr;31(4):590-601. doi: 10.1016/j.hlc.2021.08.026. Epub 2021 Oct 28. Heart Lung Circ. 2022. PMID: 34756532
-
Systematic review and meta-analysis of mortality risk prediction models in adult cardiac surgery.Interact Cardiovasc Thorac Surg. 2021 Oct 29;33(5):673-686. doi: 10.1093/icvts/ivab151. Interact Cardiovasc Thorac Surg. 2021. PMID: 34041539 Free PMC article.
Cited by
-
A machine learning algorithm-based risk prediction score for in-hospital/30-day mortality after adult cardiac surgery.Eur J Cardiothorac Surg. 2024 Oct 1;66(4):ezae368. doi: 10.1093/ejcts/ezae368. Eur J Cardiothorac Surg. 2024. PMID: 39374541 Free PMC article.
-
Machine Learning Methods for Predicting Long-Term Mortality in Patients After Cardiac Surgery.Front Cardiovasc Med. 2022 May 3;9:831390. doi: 10.3389/fcvm.2022.831390. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35592400 Free PMC article.
-
Artificial Intelligence-enabled Decision Support in Surgery: State-of-the-art and Future Directions.Ann Surg. 2023 Jul 1;278(1):51-58. doi: 10.1097/SLA.0000000000005853. Epub 2023 Mar 21. Ann Surg. 2023. PMID: 36942574 Free PMC article.
-
Diachronic and synchronic variation in the performance of adaptive machine learning systems: the ethical challenges.J Am Med Inform Assoc. 2023 Jan 18;30(2):361-366. doi: 10.1093/jamia/ocac218. J Am Med Inform Assoc. 2023. PMID: 36377970 Free PMC article.
-
Pre-operative Machine Learning for Heart Transplant Patients Bridged with Temporary Mechanical Circulatory Support.J Cardiovasc Dev Dis. 2022 Sep 19;9(9):311. doi: 10.3390/jcdd9090311. J Cardiovasc Dev Dis. 2022. PMID: 36135456 Free PMC article.
References
-
- Nilsson J, Algotsson L, Höglund P, Lührs C, Brandt J. Comparison of 19 preoperative risk stratification models in open-heart surgery. Eur Heart J. 2006;27:867–74. - PubMed
-
- O’Brien SM, Feng L, He X, Xian Y, Jacobs IP, Badhwar V, et al. The Society of Thoracic Surgeons 2018 adult cardiac surgery risk models: part 2-statistical methods and results. Ann Thorac Surg. 2018;105:1419–28. - PubMed
-
- Kilic A, Goyal A, Miller JK, Gjekmarkaj E, Tam WL, Gleason TG, et al. Predictive utility of a machine learning algorithm in estimating mortality risk in cardiac surgery. Ann Thorac Surg. 2020;109:1811–9. - PubMed
-
- D’Agostino RS, Jacobs JP, Badhwar V, Fernandez FG, Paone G, Wormuth DW, et al. The Society of Thoracic Surgeons adult cardiac surgery database: 2018 update on outcomes and quality. Ann Thorac Surg. 2018;105:15–23. - PubMed
-
- Shahian DM, Jacobs JP, Badhwar V, Kurlansky PA, Furnary AP, Cleveland JC Jr, et al. The Society of Thoracic Surgeons 2018 adult cardiac surgery risk models: part 1-background, design considerations, and model development. Ann Thorac Surg. 2018;105:1411–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
