

Incidence and mortality rates of keratinocyte carcinoma from 1998-2017: a population-based study of sex differences in Ontario, Canada
- PMID: 34607845
- PMCID: PMC8568084
- DOI: 10.1503/cmaj.210595
Incidence and mortality rates of keratinocyte carcinoma from 1998-2017: a population-based study of sex differences in Ontario, Canada
Abstract
Background: Keratinocyte carcinoma is the most common malignant disease, but it is not captured in major registries. We aimed to describe differences by sex in the incidence and mortality rates of keratinocyte carcinoma in Ontario, Canada.
Methods: We conducted a population-based retrospective study of adults residing in Ontario between Jan. 1, 1998, and Dec. 31, 2017, using linked health administrative databases. We identified the first diagnosis of keratinocyte carcinoma using a validated algorithm of health insurance claims, and deaths related to keratinocyte carcinoma from death certificates. We calculated the incidence and mortality rates of keratinocyte carcinoma, stratified by sex, age and income quintile. We evaluated trends using the average annual percentage change (AAPC) based on joinpoint regression.
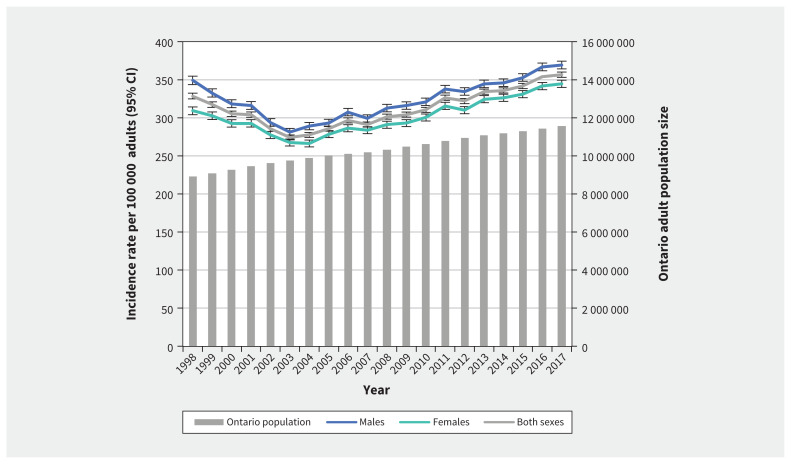
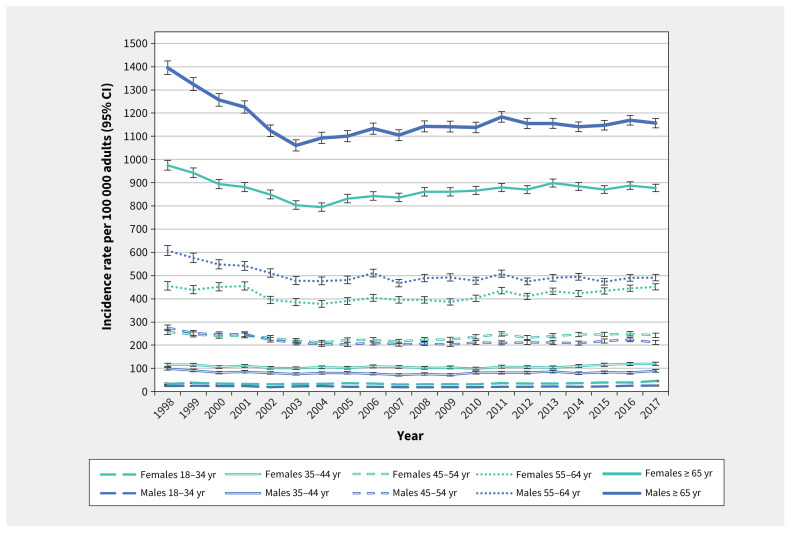
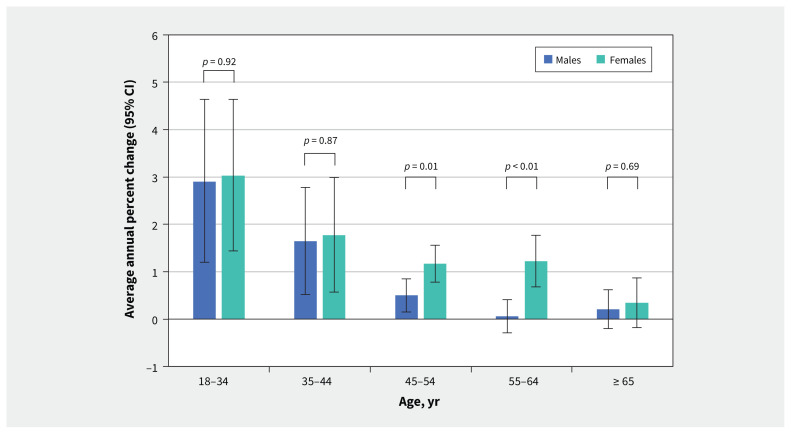
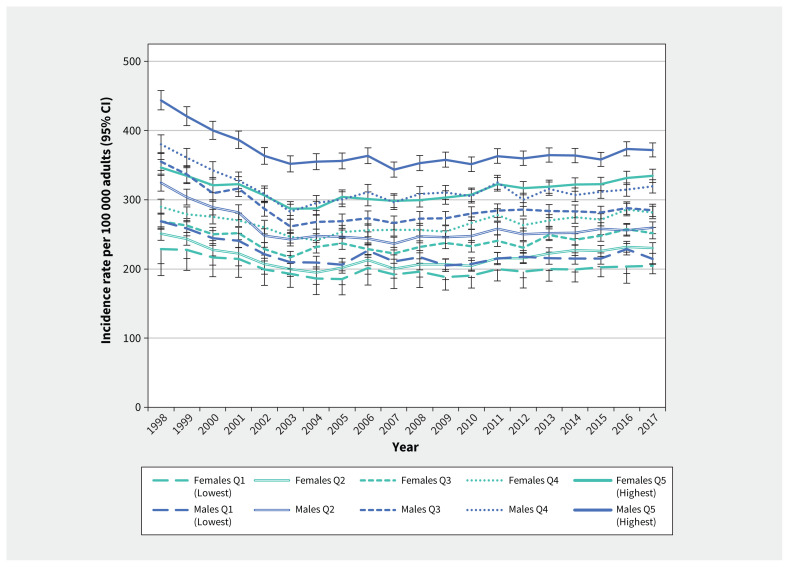
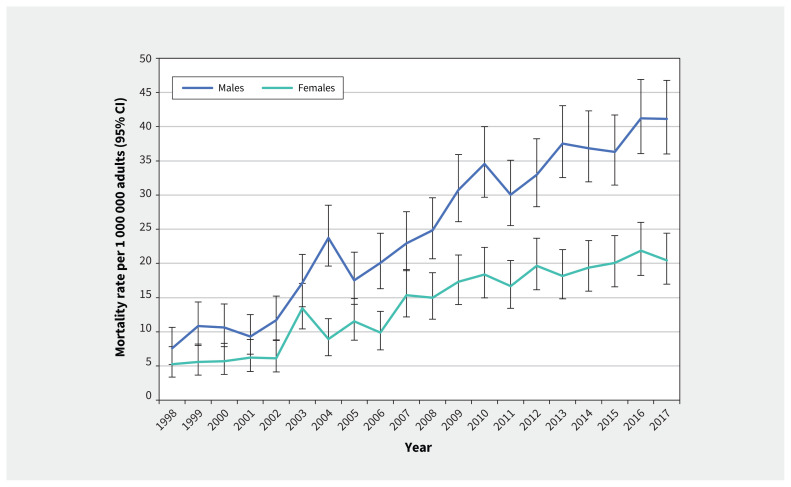
Results: After decreasing from 1998 to 2003, the incidence rate of keratinocyte carcinoma increased by 30% to 369 per 100 000 males and 345 per 100 000 females in 2017 (AAPC 1.9%, 95% confidence interval [CI] 1.7 to 2.1 from 2003 to 2017). The incidence rate was higher in females younger than 55 years, but higher in males aged 55 years or older. Between 2008 and 2017, the incidence rate rose faster in females than males aged 45-54 years (AAPC 1.2% v. 0.5%, p = 0.01) and 55-64 years (1.2% v. 0.1%, p < 0.01). The incidence was higher in males than females in the higher income quintiles. Between 1998 and 2017, the mortality rate of keratinocyte carcinoma was 1.8 times higher in males than females, on average, and rose 4.8-fold overall (AAPC 8.9%, 95% CI 6.4 to 11.4 in males; 8.0%, 95% CI 5.3-10.8 in females).
Interpretation: The population burden of keratinocyte carcinoma is growing, and the incidence and mortality rates rose disproportionately among certain sex- and age-specific groups. This warrants further investigation into causal factors and renewed preventive public health measures.
© 2021 CMA Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: An-Wen Chan reports funding from Pellepharm to his institution to support participation as a clinical trial site, outside the submitted work. No other competing interests were declared.
Figures
Similar articles
-
Application of Recursive Partitioning to Derive and Validate a Claims-Based Algorithm for Identifying Keratinocyte Carcinoma (Nonmelanoma Skin Cancer).JAMA Dermatol. 2016 Oct 1;152(10):1122-1127. doi: 10.1001/jamadermatol.2016.2609. JAMA Dermatol. 2016. PMID: 27533718
-
Age group-specific changes in keratinocyte cancer treatment rates in Australia, 2012-2021: a retrospective cohort study based on MBS claims data.Med J Aust. 2024 May 20;220(9):472-479. doi: 10.5694/mja2.52293. Epub 2024 Apr 29. Med J Aust. 2024. PMID: 38685827
-
Association of Age, Sex, Race, and Geographic Region With Variation of the Ratio of Basal Cell to Cutaneous Squamous Cell Carcinomas in the United States.JAMA Dermatol. 2020 Nov 1;156(11):1192-1198. doi: 10.1001/jamadermatol.2020.2571. JAMA Dermatol. 2020. PMID: 32845319 Free PMC article.
-
Trends in Non-Melanoma Skin Cancer (Basal Cell Carcinoma and Squamous Cell Carcinoma) in Canada: A Descriptive Analysis of Available Data.J Cutan Med Surg. 2016 Mar-Apr;20(2):166-75. doi: 10.1177/1203475415610106. Epub 2015 Oct 12. J Cutan Med Surg. 2016. PMID: 26458408 Review.
-
Trends in the population-based incidence of squamous cell carcinoma of the skin first diagnosed between 1984 and 1992.Arch Dermatol. 1997 Jun;133(6):735-40. Arch Dermatol. 1997. PMID: 9197827 Review.
Cited by
-
Uncovering the complex relationship between balding, testosterone and skin cancers in men.Nat Commun. 2023 Oct 3;14(1):5962. doi: 10.1038/s41467-023-41231-8. Nat Commun. 2023. PMID: 37789011 Free PMC article.
-
Skin Cancer Prevention across the G7, Australia and New Zealand: A Review of Legislation and Guidelines.Curr Oncol. 2023 Jun 23;30(7):6019-6040. doi: 10.3390/curroncol30070450. Curr Oncol. 2023. PMID: 37489567 Free PMC article. Review.
-
Skin Cancer Pathobiology at a Glance: A Focus on Imaging Techniques and Their Potential for Improved Diagnosis and Surveillance in Clinical Cohorts.Int J Mol Sci. 2023 Jan 5;24(2):1079. doi: 10.3390/ijms24021079. Int J Mol Sci. 2023. PMID: 36674595 Free PMC article. Review.
-
Top 10 research priorities for cutaneous squamous cell carcinoma: results of the Skin Investigation Network of Canada Priority Setting Initiative.Br J Dermatol. 2024 Feb 16;190(3):431-432. doi: 10.1093/bjd/ljad387. Br J Dermatol. 2024. PMID: 38114099 Free PMC article.
-
High-throughput lipidomic profiles sampled with electroporation-based biopsy differentiate healthy skin, cutaneous squamous cell carcinoma, and basal cell carcinoma.Skin Res Technol. 2024 May;30(5):e13706. doi: 10.1111/srt.13706. Skin Res Technol. 2024. PMID: 38721854 Free PMC article.
References
-
- Karimkhani C, Boyers LN, Dellavalle RP, et al. . It’s time for “keratinocyte carcinoma” to replace the term “nonmelanoma skin cancer”. J Am Acad Dermatol 2015;72:186–7. - PubMed
-
- McLean DI, Phillips N, Zhou Y, et al. . 40-year trends in skin cancer in British Columbia, Canada, 1973 to 2003. J Cutan Med Surg 2012;16:83–91. - PubMed
-
- Pilgrim W, Hayes R, Hanson DW, et al. . Skin cancer (basal cell carcinoma, squamous cell carcinoma, and malignant melanoma): new cases, treatment practice, and health care costs in New Brunswick, Canada, 2002–2010. J Cutan Med Surg 2014;18:320–31. - PubMed
-
- Lim HW, Collins SAB, Resneck JS, Jr, et al. . The burden of skin disease in the United States. J Am Acad Dermatol 2017;76:958–972.e2. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials