

Development of a Simplified Patient-Centered Pelvic Floor Surgery Complication Scale
- PMID: 34608035
- PMCID: PMC9164991
- DOI: 10.1097/SPV.0000000000001099
Development of a Simplified Patient-Centered Pelvic Floor Surgery Complication Scale
Abstract
Objectives: There does not currently exist a complication scale to evaluate pelvic reconstructive surgery (PRS) that takes in account patient-centered outcomes. The purpose of this study was to characterize and compare patient and surgeon responses to a simplified, patient-centered version of the previously described Pelvic Floor Complication Scale (PFCS).
Methods: This is a multicenter (4 female pelvic medicine and reconstructive surgery practices) cross-sectional study of patients and surgeons. Using focus groups and telephone surveys, the original PFCS questionnaire was simplified. One hundred and twenty-four patients were recruited 6-12 months after PRS. Fifty-seven surgeons were recruited via electronic questionnaires. Surgeons and patients were asked to rank the severity and bother of each complication on a scale of 0 to 5 (0, none; 1, mild; 3, moderate; 5, major).
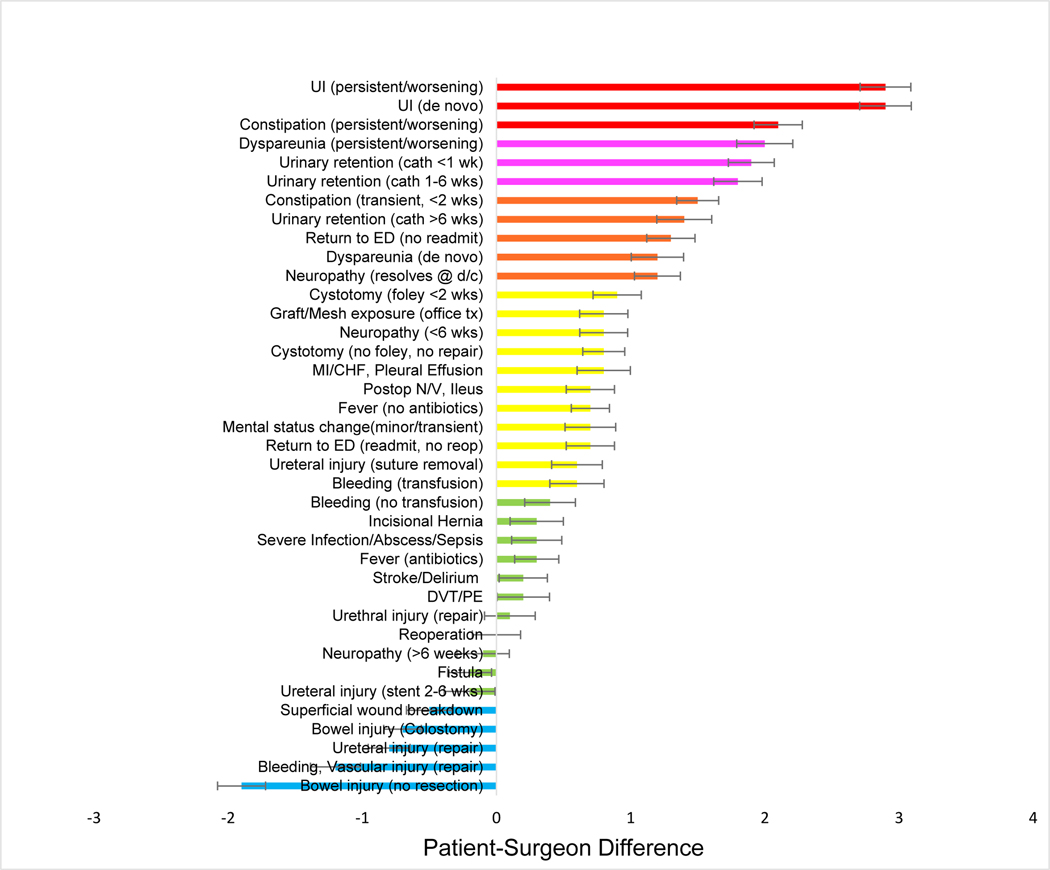
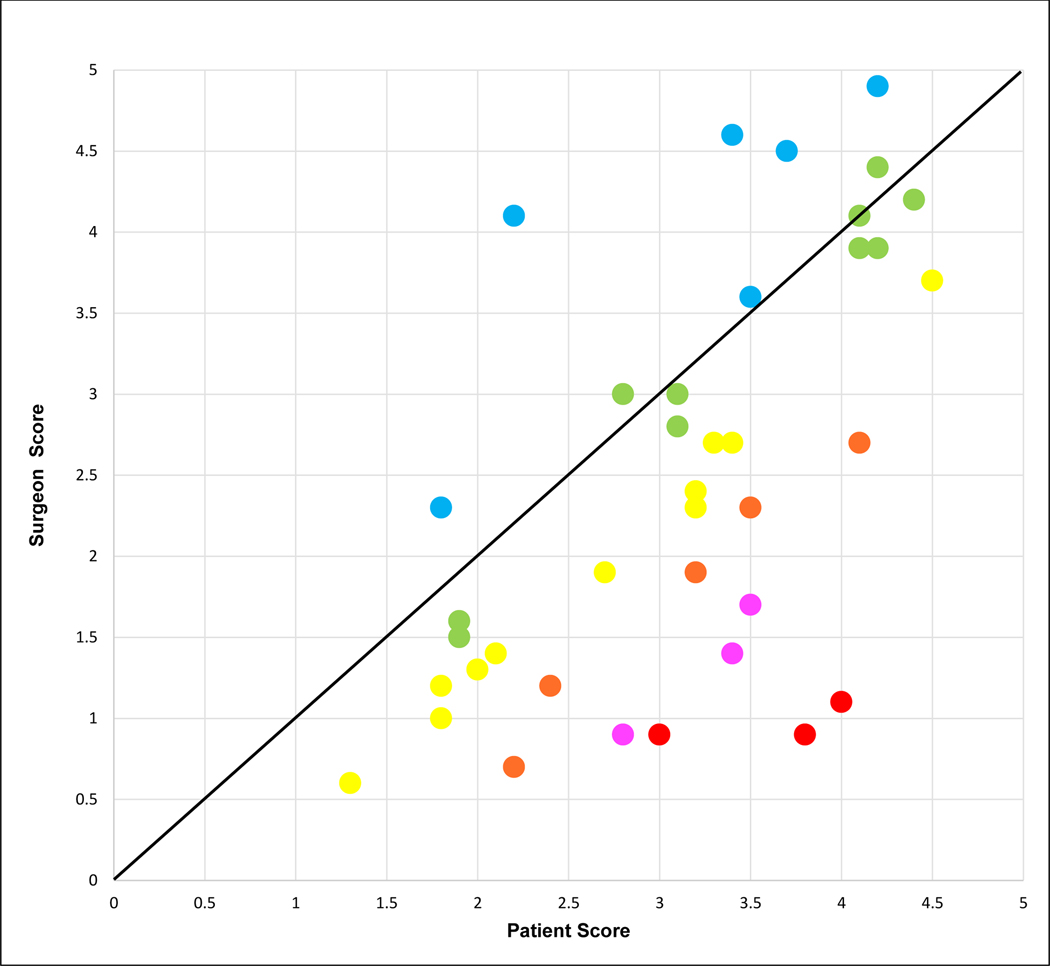
Results: Patients rated bother higher than severity for 36 of 38 complications (all differences ≤0.5 points). For statistical analysis, the highest response to patient bother/severity was chosen to weigh in favor of the patient. Patient bother/severity scores were significantly different (±0.5 points) for 27 of 38 complications compared with surgeon responses. Surgeon scores were higher for 5 complications (0.5-1.9 point differences) related to major injury requiring repair and wound breakdown. Patient scores were higher for 22 complications with the highest differences related to dyspareunia, constipation, or new/persistent urinary incontinence.
Conclusions: This mixed methods investigation revealed key differences between how patients and surgeons value PRS complications. Surgeons scored major surgical injuries higher than patients, whereas patients rated issues that many surgeons consider quality-of-life outcomes higher due to potential long-term bother. These data will be used to create a simplified, patient-centered PFCS.
Copyright © 2021 American Urogynecologic Society. All rights reserved.
Conflict of interest statement
The authors have declared they have no conflicts of interest.
Figures

References
-
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
