

Real-world experience of CPX-351 as first-line treatment for patients with acute myeloid leukemia
- PMID: 34608129
- PMCID: PMC8490353
- DOI: 10.1038/s41408-021-00558-5
Real-world experience of CPX-351 as first-line treatment for patients with acute myeloid leukemia
Abstract
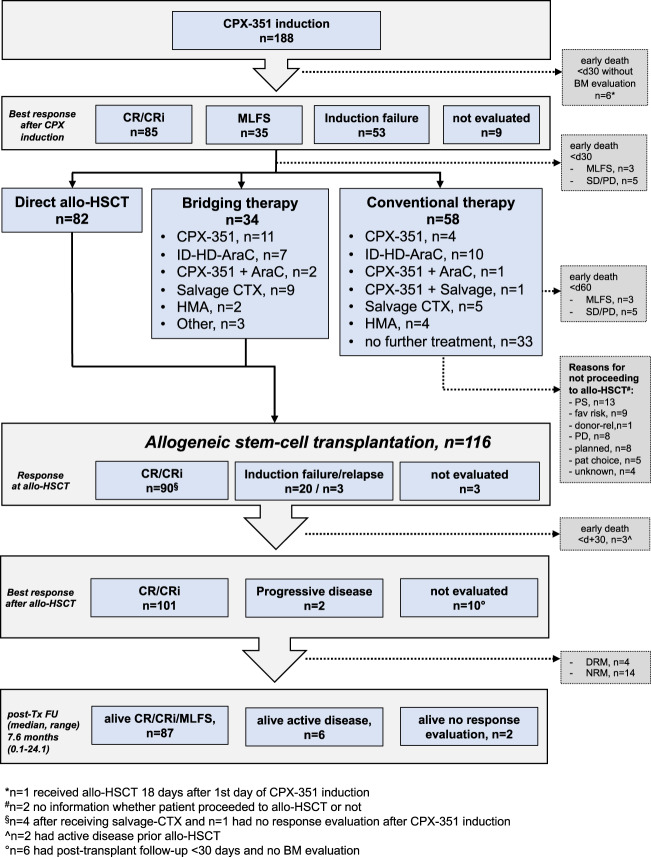
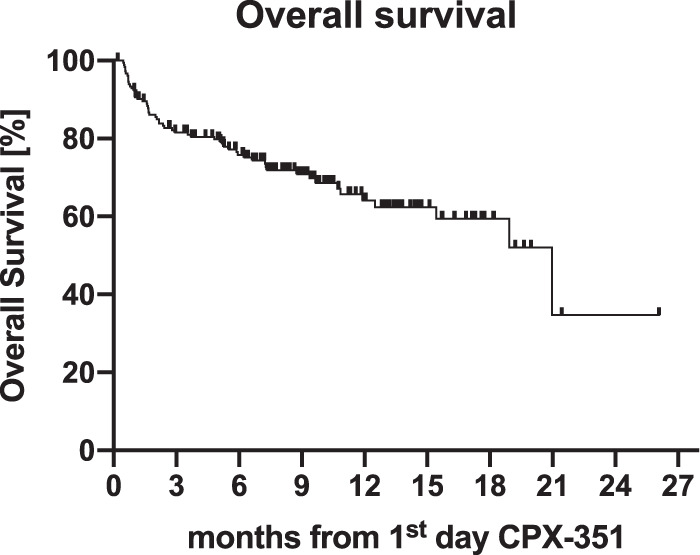
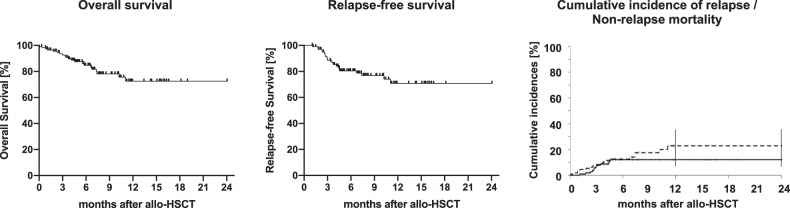
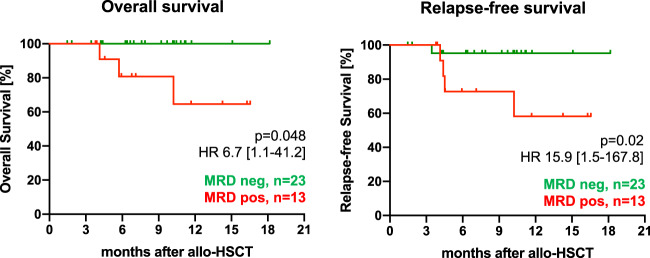
To investigate the efficacy and toxicities of CPX-351 outside a clinical trial, we analyzed 188 patients (median age 65 years, range 26-80) treated for therapy-related acute myeloid leukemia (t-AML, 29%) or AML with myelodysplasia-related changes (AML-MRC, 70%). Eighty-six percent received one, 14% two induction cycles, and 10% received consolidation (representing 22% of patients with CR/CRi) with CPX-351. Following induction, CR/CRi rate was 47% including 64% of patients with available information achieving measurable residual disease (MRD) negativity (<10-3) as measured by flow cytometry. After a median follow-up of 9.3 months, median overall survival (OS) was 21 months and 1-year OS rate 64%. In multivariate analysis, complex karyotype predicted lower response (p = 0.0001), while pretreatment with hypomethylating agents (p = 0.02) and adverse European LeukemiaNet 2017 genetic risk (p < 0.0001) were associated with lower OS. Allogeneic hematopoietic cell transplantation (allo-HCT) was performed in 116 patients (62%) resulting in promising outcome (median survival not reached, 1-year OS 73%), especially in MRD-negative patients (p = 0.048). With 69% of patients developing grade III/IV non-hematologic toxicity following induction and a day 30-mortality of 8% the safety profile was consistent with previous findings. These real-world data confirm CPX-351 as efficient treatment for these high-risk AML patients facilitating allo-HCT in many patients with promising outcome after transplantation.
© 2021. The Author(s).
Conflict of interest statement
T Schroeder: advisory boards, lecture fees from JAZZ Pharmaceuticals Germany. JMM: personal fee, advisory board from JAZZ Pharmaceuticals Germany. HD: Advisory Board with honoraria: AbbVie, Agios, Amgen, Astellas, Astex Pharmaceuticals, AstraZeneca, Berlin-Chemie, BMS, Celgene, GEMoaB, Gilead, Helsinn, Janssen, Jazz, Novartis, Oxford Biomedica, Roche; clinical research funding: Agios, Amgen, Astellas, Bristol Myers Squibb, Celgene, Jazz Pharmaceuticals, Novartis, Pfizer. KG: Advisory Board with honoraria: AbbVie, JAZZ, BMS/Celgene Deutschland GmbH, Alexion; research funding: BMS/Celgene. T Sauer: Advisory Board with honoraria: AbbVie, Takeda, Astellas. CR: financial travel support: JAZZ Pharmeceuticals and BMS/Celgene Deutschland GmbH; lecture fees: BMS/Celgene Deutschland GmbH. GK: received lecture fees from BMS/Celgene Deutschland GmbH, Novartis, Jazz Pharmaceuticals and Janssen-Cilag GmbH. FS: advisory board with honoraria: JAZZ Pharmaceuticals, AbbVie, medac GmbH. Ulrich Germing: research funding: BMS/Celgene Deutschland GmbH, Novartis.
Figures
References
-
- Nagel G, Weber D, Fromm E, Erhardt S, Lübbert M, Fiedler W, et al. German-Austrian AML Study Group (AMLSG) Epidemiological, genetic, and clinical characterization by age of newly diagnosed acute myeloid leukemia based on an academic population-based registry study (AMLSG BiO) Ann Hematol. 2017;96:1993–2003. doi: 10.1007/s00277-017-3150-3. - DOI - PMC - PubMed
-
- Hulegårdh E, Nilsson C, Lazarevic V, Garelius H, Antunovic P, Rangert Derolf Å, et al. Characterization and prognostic features of secondary acute myeloid leukemia in a population-based setting: a report from the Swedish Acute Leukemia Registry. Am J Hematol. 2015;90:208–14. doi: 10.1002/ajh.23908. - DOI - PubMed
-
- Granfeldt Østgård LS, Medeiros BC, Sengeløv H, Nørgaard M, Andersen MK, Dufva IH, et al. Epidemiology and clinical significance of secondary and therapy-related acute myeloid leukemia: a national population-based cohort study. J Clin Oncol. 2015;33:3641–9. doi: 10.1200/JCO.2014.60.0890. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
