

Closed-loop neuromodulation in an individual with treatment-resistant depression
- PMID: 34608328
- PMCID: PMC11219029
- DOI: 10.1038/s41591-021-01480-w
Closed-loop neuromodulation in an individual with treatment-resistant depression
Abstract
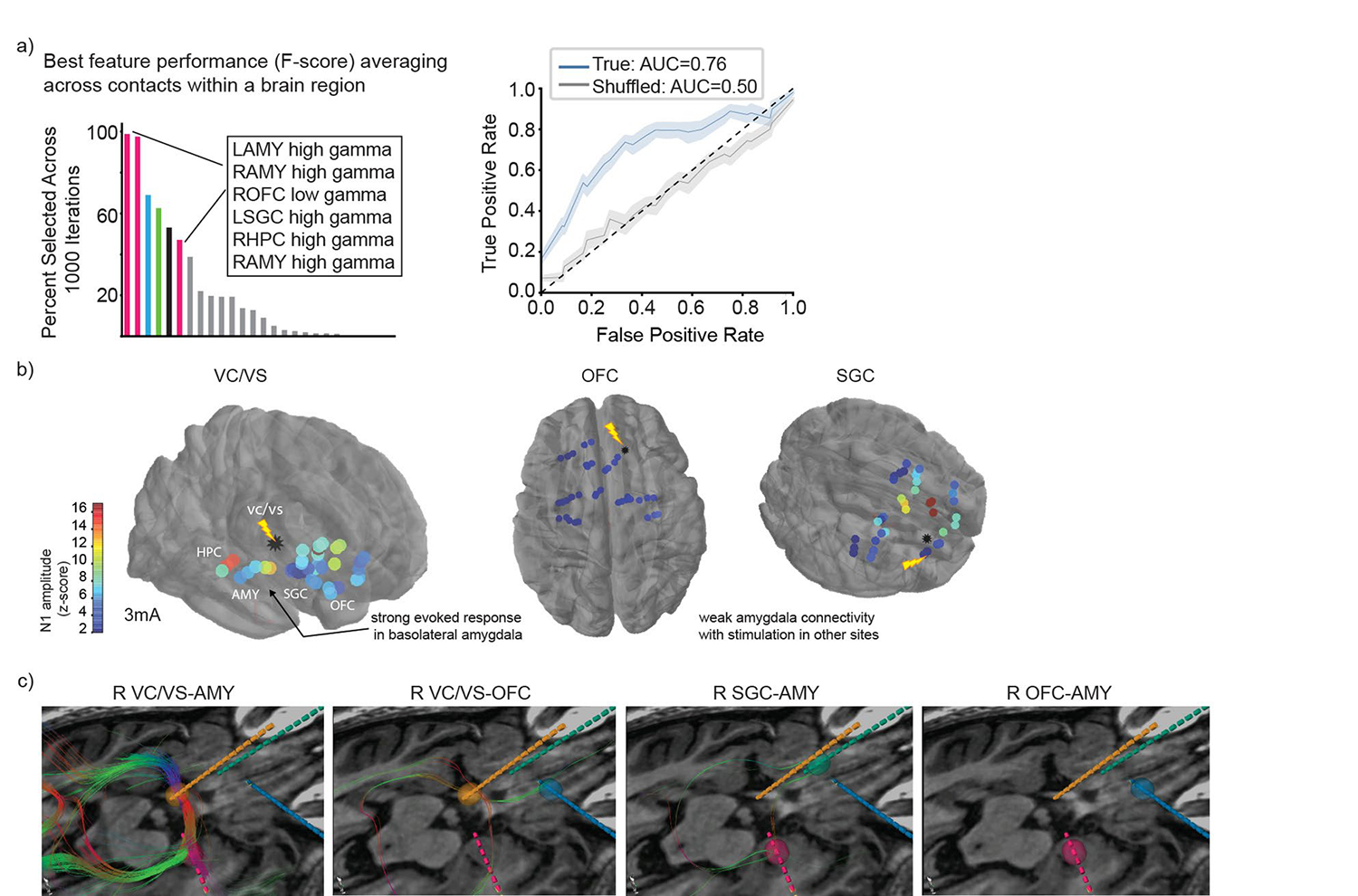
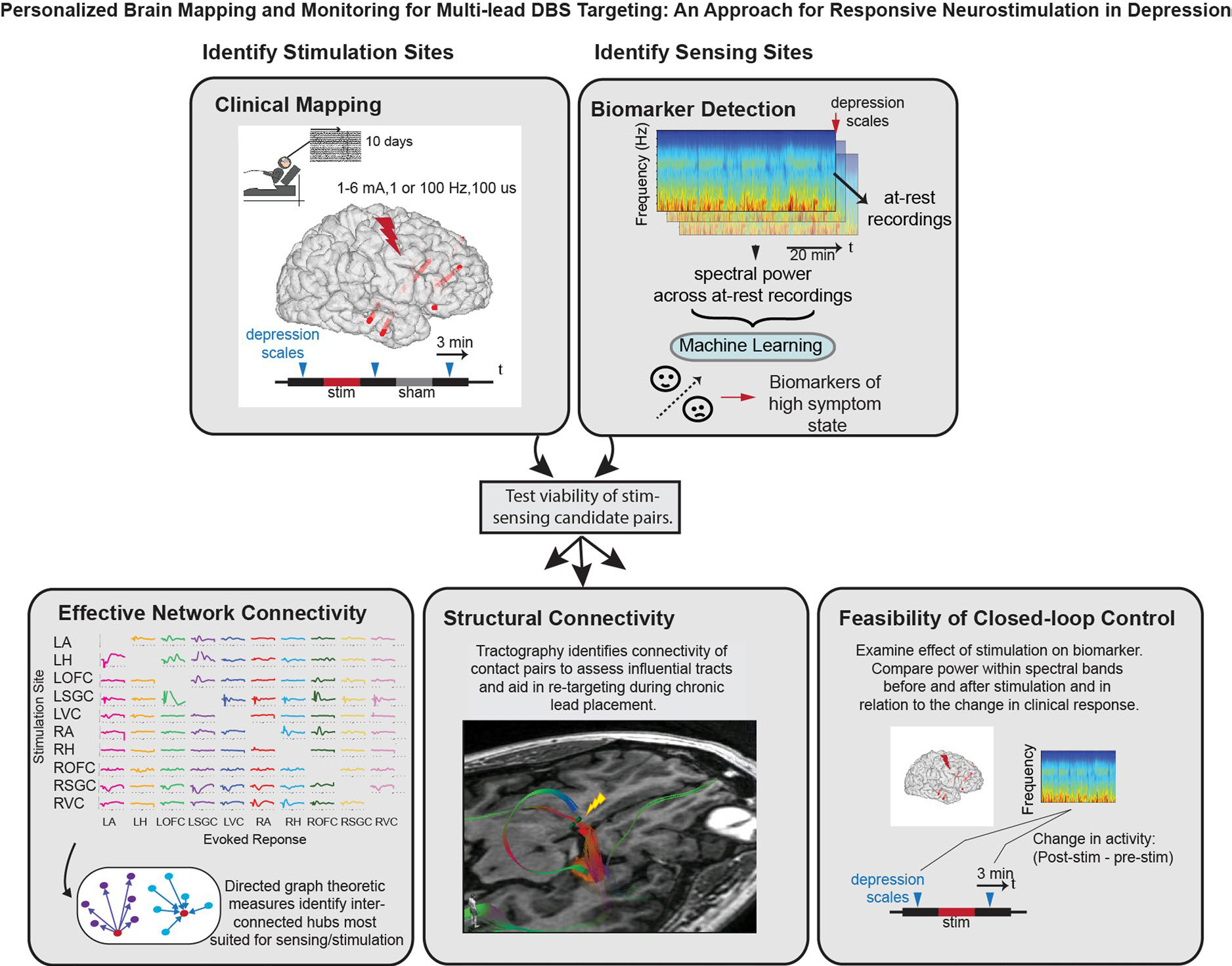
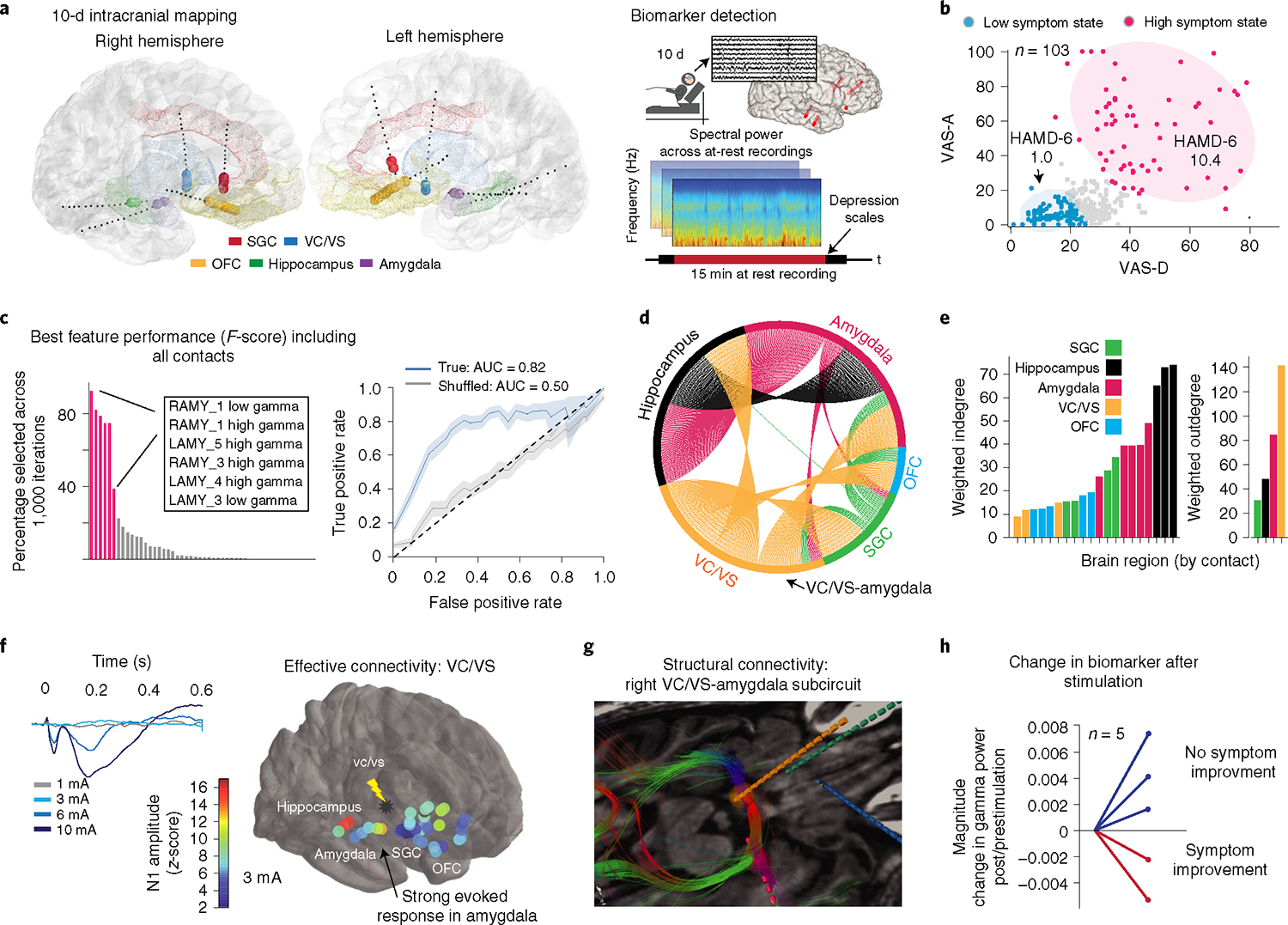
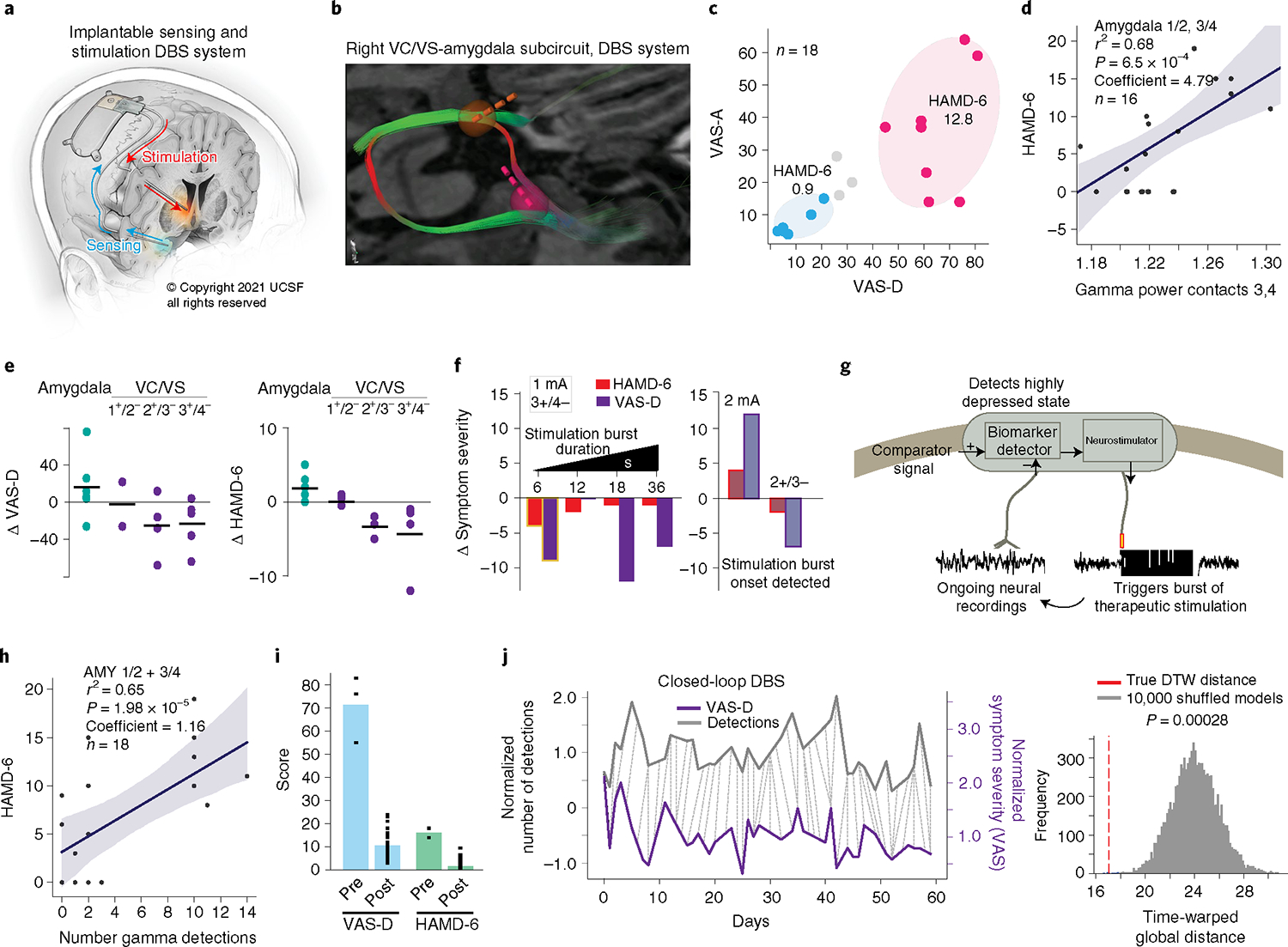
Deep brain stimulation is a promising treatment for neuropsychiatric conditions such as major depression. It could be optimized by identifying neural biomarkers that trigger therapy selectively when symptom severity is elevated. We developed an approach that first used multi-day intracranial electrophysiology and focal electrical stimulation to identify a personalized symptom-specific biomarker and a treatment location where stimulation improved symptoms. We then implanted a chronic deep brain sensing and stimulation device and implemented a biomarker-driven closed-loop therapy in an individual with depression. Closed-loop therapy resulted in a rapid and sustained improvement in depression. Future work is required to determine if the results and approach of this n-of-1 study generalize to a broader population.
© 2021. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing interests
A.D.K. consults for Eisai, Evecxia Therapeutics, Ferring Pharmaceuticals, Galderma, Harmony Biosciences, Idorsia, Jazz Pharmaceuticals, Janssen Pharmaceuticals, Merck, Neurocrine Biosciences, Pernix Pharma, Sage Therapeutics, Takeda Pharmaceutical Company, Big Health, Millennium Pharmaceuticals, Otsuka Pharmaceutical and Neurawell Therapeutics. A.D.K. acknowledges support from Janssen Pharmaceuticals, Jazz Pharmaceuticals, Axsome Therapeutics (no. AXS-05–301) and Reveal Biosensors. K.W.S. serves on the advisory board of Nesos. UCSF and E.F.C. have patents related to brain stimulation for the treatment of neuropsychiatric disorders. V.R.R. has served as a paid consultant for NeuroPace but declares no targeted funding from NeuroPace for this study. P.A.S. receives research support from Medtronic. The other authors declare no competing interests.
Figures
References
-
- Howland RH Sequenced Treatment Alternatives to Relieve Depression (STAR*D). Part 2: study outcomes. J. Psychosoc. Nurs. Ment. Health Serv 46, 21–24 (2008). - PubMed
-
- Holtzheimer PE et al. Subcallosal cingulate deep brain stimulation for treatment-resistant depression: a multisite, randomised, sham-controlled trial. Lancet Psychiatry 4, 839–849 (2017). - PubMed
-
- Dougherty DD et al. A randomized sham-controlled trial of deep brain stimulation of the ventral capsule/ventral striatum for chronic treatment-resistant depression. Biol. Psychiatry 78, 240–248 (2015). - PubMed
-
- Bergfeld IO et al. Deep brain stimulation of the ventral anterior limb of the internal capsule for treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry 73, 456–464 (2016). - PubMed
