

Diagnosis of sarcopenia by evaluating skeletal muscle mass by adjusted bioimpedance analysis validated with dual-energy X-ray absorptiometry
- PMID: 34609065
- PMCID: PMC8718029
- DOI: 10.1002/jcsm.12825
Diagnosis of sarcopenia by evaluating skeletal muscle mass by adjusted bioimpedance analysis validated with dual-energy X-ray absorptiometry
Abstract
Background: This study aimed to adjust and cross-validate skeletal muscle mass measurements between bioimpedance analysis (BIA) and dual-energy X-ray absorptiometry (DXA) for the screening of sarcopenia in the community and to estimate the prevalence of sarcopenia in Hong Kong.
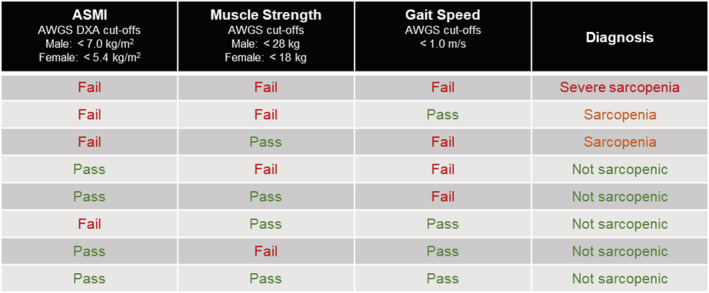
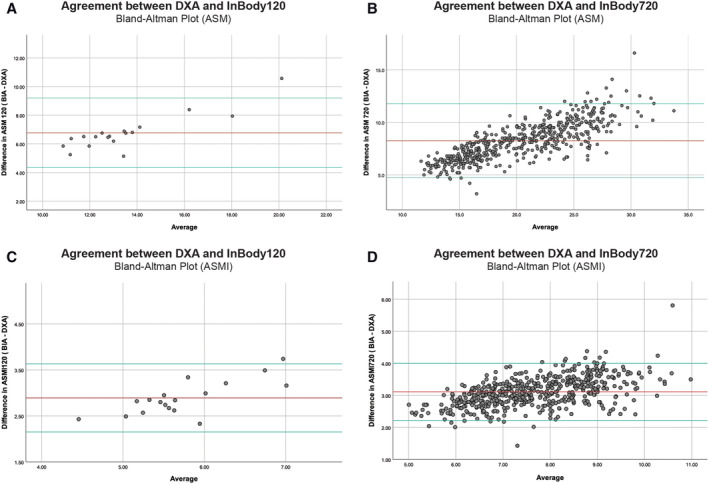
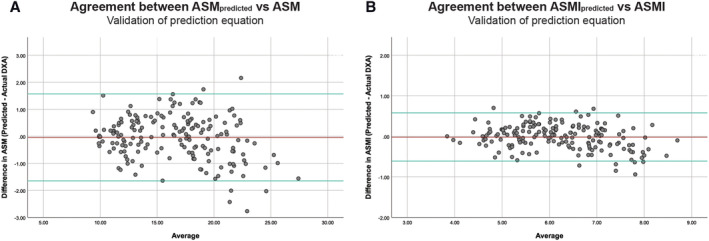
Methods: Screening of sarcopenia was provided to community-dwelling older adults. Appendicular skeletal muscle mass (ASM) was evaluated by BIA (InBody 120 or 720) and/or DXA. Handgrip strength and/or gait speed were assessed. Diagnosis of sarcopenia was based on the 2019 revised Asian Working Group for Sarcopenia cut-offs. Agreement analysis was performed to cross-validate ASM measurements by BIA and DXA. Multiple regression was used to explore contribution of measured parameters in predicting DXA ASM from BIA.
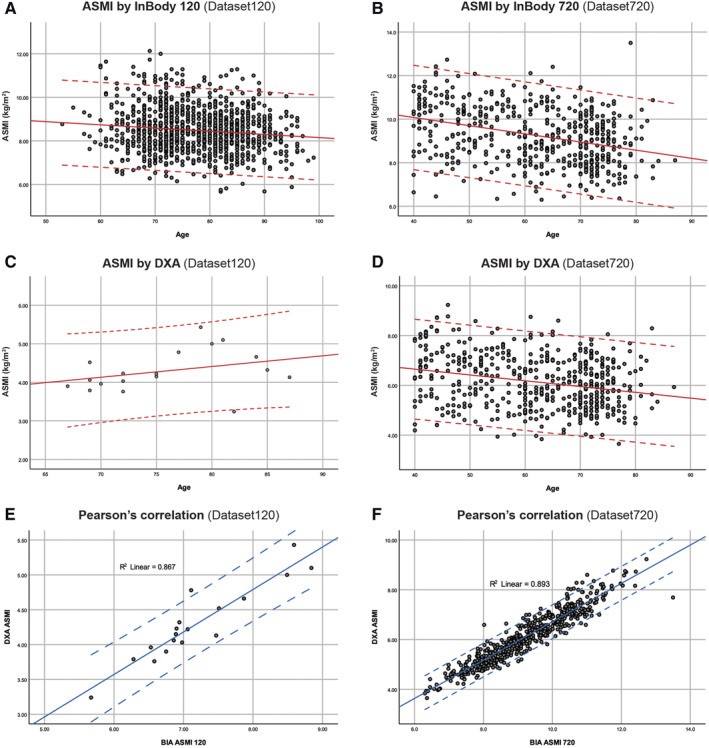
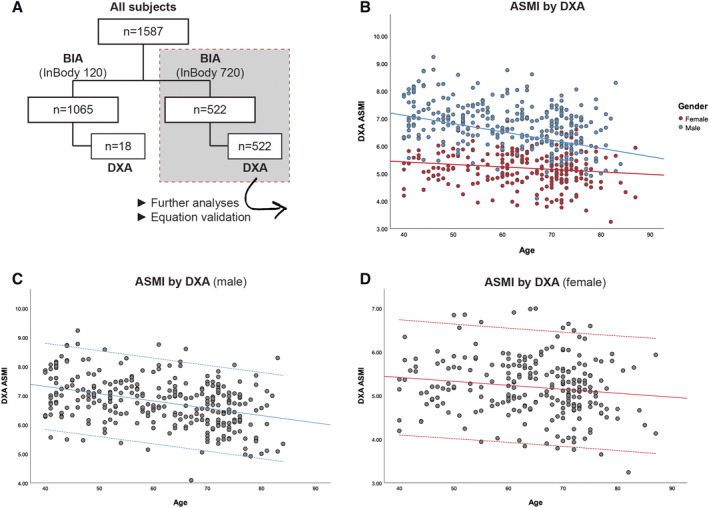
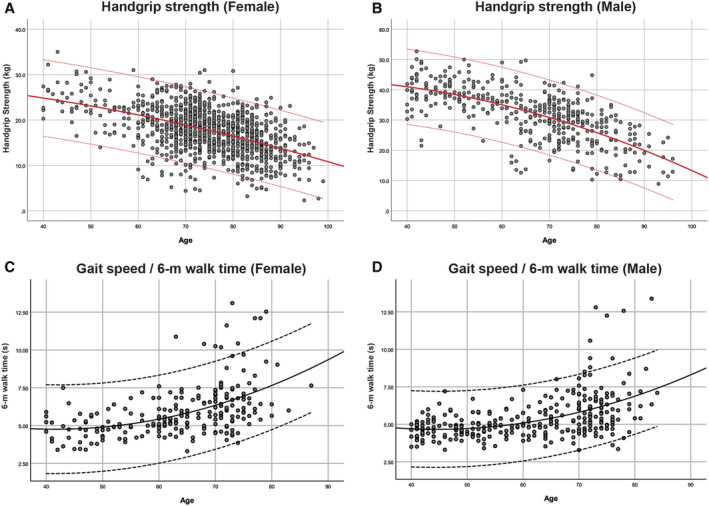
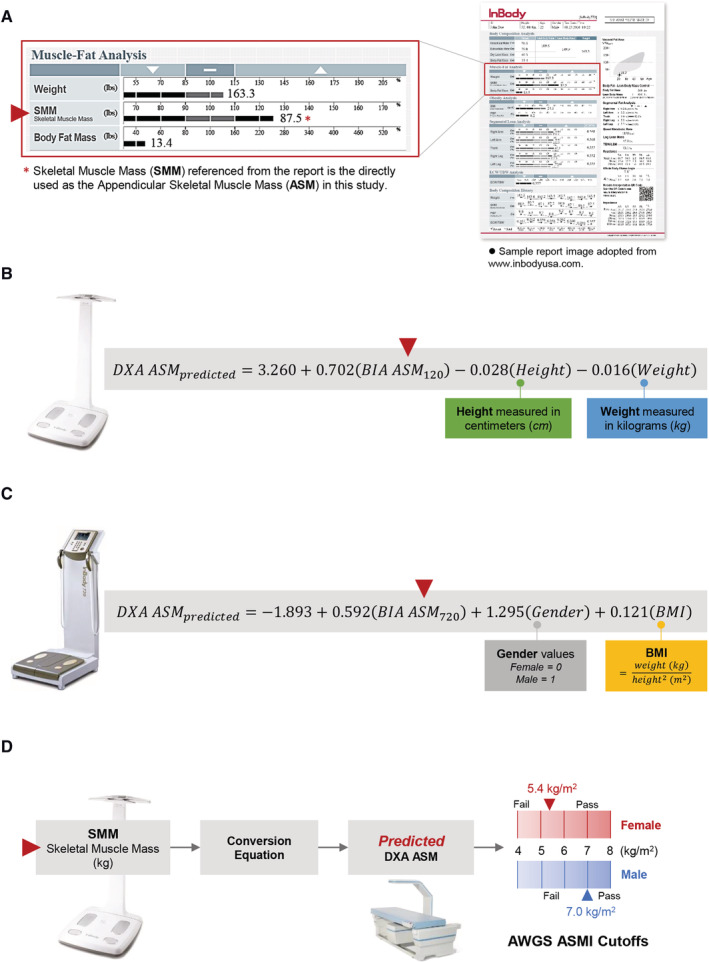
Results: A total of 1587 participants (age = 72 ± 12 years) were recruited; 1065 participants were screened by BIA (InBody 120) with 18 followed up by DXA, while the remaining 522 participants were assessed by the BIA (InBody 720) and DXA. The appendicular skeletal muscle mass index (ASMI) evaluated by BIA showed a mean difference of 2.89 ± 0.38 kg/m2 (InBody 120) and 2.97 ± 0.45 kg/m2 (InBody 720) against DXA gold standard. A significant overestimation of muscle mass was measured by BIA compared with DXA (P < 0.005). BIA data were adjusted using prediction equation and mean difference reduced to -0.02 ± 0.31 kg/m2 in cross-validation. Prevalence of sarcopenia in older adults ≥65 ranged from 39.4% (based on ASMI by DXA) to 40.8% (based on predicted DXA ASMI from BIA). Low ASMI by DXA was found in 68.5% of the older adults screened. The percentage of older adults exhibited low handgrip strength ranged from 31.3% to 56%, while 49% showed low gait speed.
Conclusions: Bioimpedance analysis was found to overestimate skeletal muscle mass compared with DXA. With adjustment equations, BIA can be used as a quick and reliable tool for screening sarcopenia in community and clinical settings with limited access to better options.
Keywords: Bioimpedance analysis (BIA); Diagnosis; Dual-energy X-ray absorptiometry (DXA); Sarcopenia; Skeletal muscle mass.
© 2021 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
None declared.
Figures
References
-
- Cruz‐Jentoft AJ, Sayer AA. Sarcopenia. Lancet 2019;393:2636–2646. - PubMed
-
- Cao L, Morley JE. Sarcopenia is recognized as an independent condition by an International Classification of Disease, Tenth Revision, Clinical Modification (ICD‐10‐CM) code. J Am Med Dir Assoc 2016;17:675–677. - PubMed
-
- Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 2014;15:95–101. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
