

Predicting Prolonged Apnea During Nurse-Administered Procedural Sedation: Machine Learning Study
- PMID: 34609322
- PMCID: PMC8527383
- DOI: 10.2196/29200
Predicting Prolonged Apnea During Nurse-Administered Procedural Sedation: Machine Learning Study
Abstract
Background: Capnography is commonly used for nurse-administered procedural sedation. Distinguishing between capnography waveform abnormalities that signal the need for clinical intervention for an event and those that do not indicate the need for intervention is essential for the successful implementation of this technology into practice. It is possible that capnography alarm management may be improved by using machine learning to create a "smart alarm" that can alert clinicians to apneic events that are predicted to be prolonged.
Objective: To determine the accuracy of machine learning models for predicting at the 15-second time point if apnea will be prolonged (ie, apnea that persists for >30 seconds).
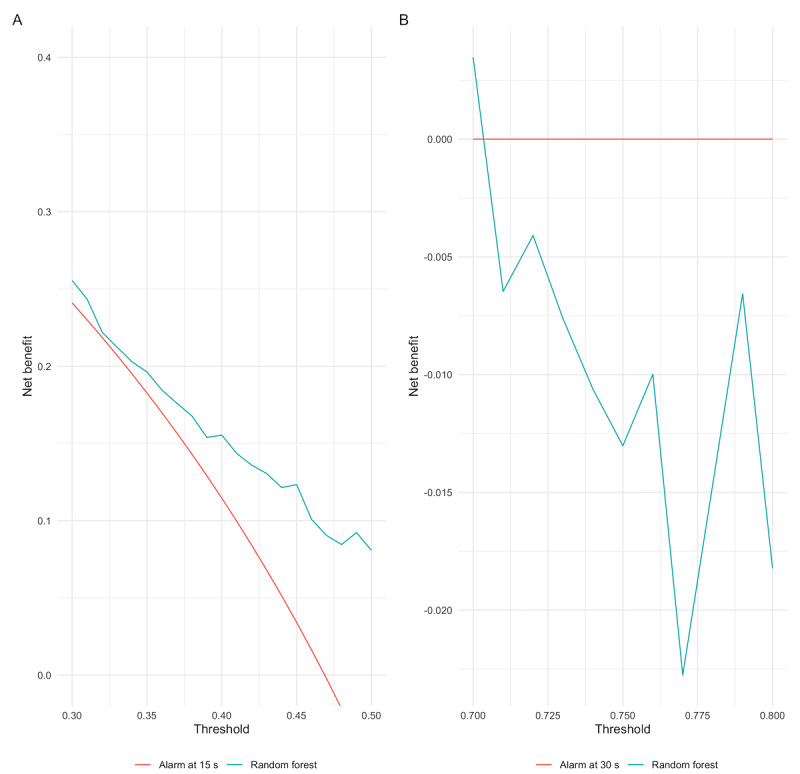
Methods: A secondary analysis of an observational study was conducted. We selected several candidate models to evaluate, including a random forest model, generalized linear model (logistic regression), least absolute shrinkage and selection operator regression, ridge regression, and the XGBoost model. Out-of-sample accuracy of the models was calculated using 10-fold cross-validation. The net benefit decision analytic measure was used to assist with deciding whether using the models in practice would lead to better outcomes on average than using the current default capnography alarm management strategies. The default strategies are the aggressive approach, in which an alarm is triggered after brief periods of apnea (typically 15 seconds) and the conservative approach, in which an alarm is triggered for only prolonged periods of apnea (typically >30 seconds).
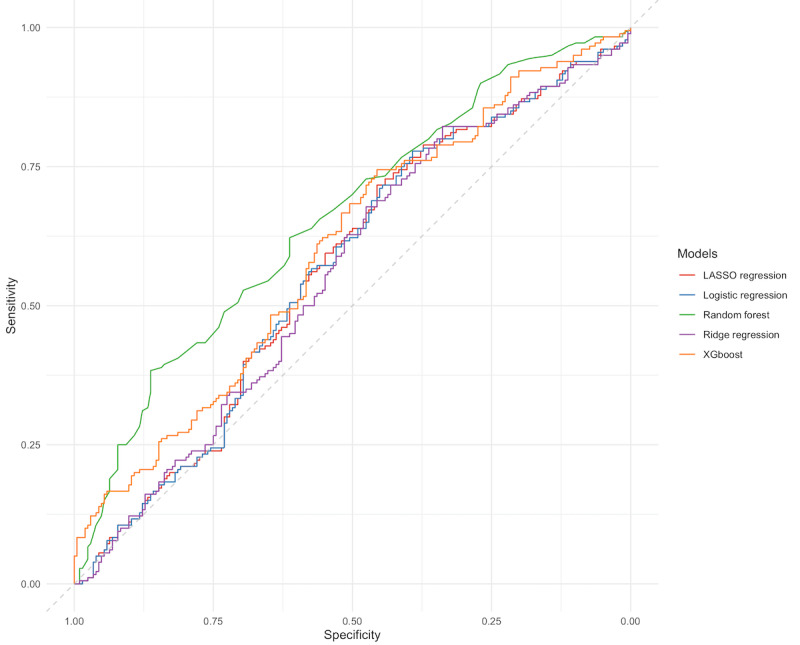
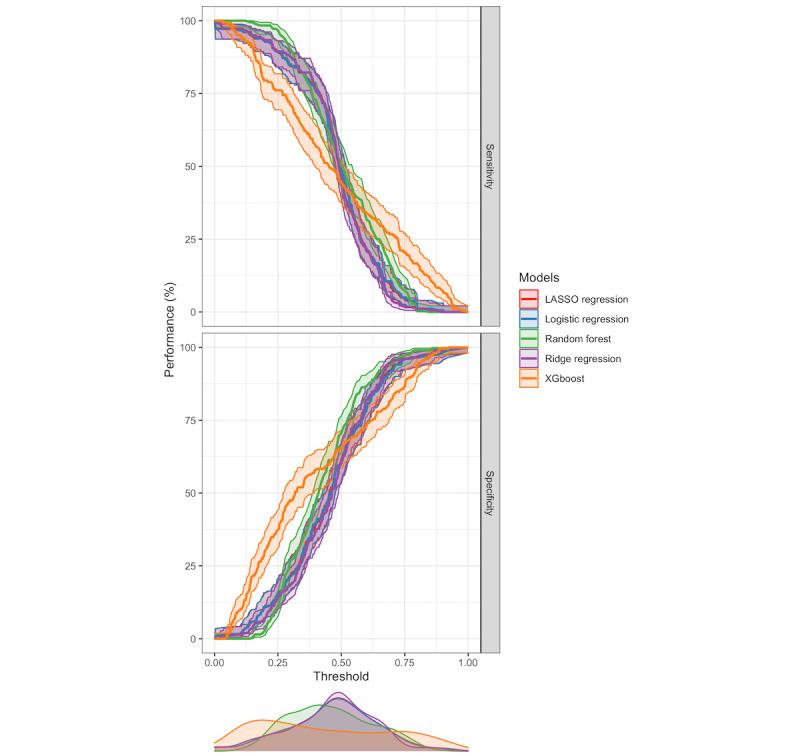
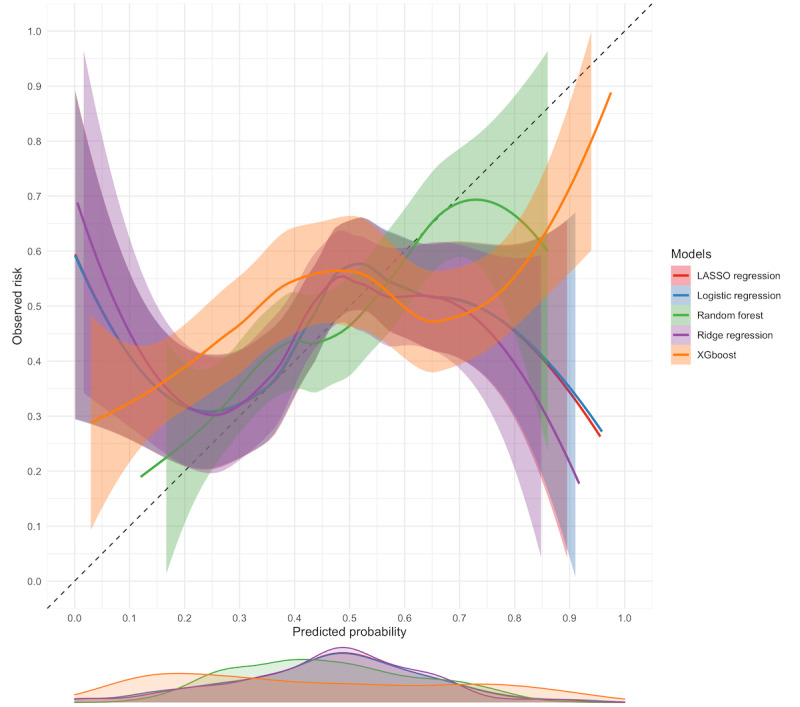
Results: A total of 384 apneic events longer than 15 seconds were observed in 61 of the 102 patients (59.8%) who participated in the observational study. Nearly half of the apneic events (180/384, 46.9%) were prolonged. The random forest model performed the best in terms of discrimination (area under the receiver operating characteristic curve 0.66) and calibration. The net benefit associated with the random forest model exceeded that associated with the aggressive strategy but was lower than that associated with the conservative strategy.
Conclusions: Decision curve analysis indicated that using a random forest model would lead to a better outcome for capnography alarm management than using an aggressive strategy in which alarms are triggered after 15 seconds of apnea. The model would not be superior to the conservative strategy in which alarms are only triggered after 30 seconds.
Keywords: anaesthesia; anesthesia; apnea; apnoea; capnography; conscious sedation; informatics; machine learning; medical informatics; nursing; patient safety; procedural sedation and analgesia; sedation; sleep apnea.
©Aaron Conway, Carla R Jungquist, Kristina Chang, Navpreet Kamboj, Joanna Sutherland, Sebastian Mafeld, Matteo Parotto. Originally published in JMIR Perioperative Medicine (http://periop.jmir.org), 05.10.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Integrated Pulmonary Index during nurse-administered procedural sedation: Study protocol for a cluster-randomized trial.J Adv Nurs. 2022 Jul;78(7):2245-2254. doi: 10.1111/jan.15243. Epub 2022 Apr 29. J Adv Nurs. 2022. PMID: 35485238
-
Pre-apneic capnography waveform abnormalities during procedural sedation and analgesia.J Clin Monit Comput. 2020 Oct;34(5):1061-1068. doi: 10.1007/s10877-019-00391-z. Epub 2019 Sep 30. J Clin Monit Comput. 2020. PMID: 31571021
-
Microstream capnography improves patient monitoring during moderate sedation: a randomized, controlled trial.Pediatrics. 2006 Jun;117(6):e1170-8. doi: 10.1542/peds.2005-1709. Epub 2006 May 15. Pediatrics. 2006. PMID: 16702250 Clinical Trial.
-
Capnography monitoring in procedural intravenous sedation: a systematic review and meta-analysis.Clin Oral Investig. 2020 Nov;24(11):3761-3770. doi: 10.1007/s00784-020-03395-1. Epub 2020 Jun 16. Clin Oral Investig. 2020. PMID: 32556657
-
Monitoring standards in sedation and analgesia: the odyssey of capnography in sedation for gastroenterology procedures.Curr Opin Anaesthesiol. 2019 Aug;32(4):453-456. doi: 10.1097/ACO.0000000000000756. Curr Opin Anaesthesiol. 2019. PMID: 31169549 Review.
Cited by
-
Decoding machine learning in nursing research: A scoping review of effective algorithms.J Nurs Scholarsh. 2025 Jan;57(1):119-129. doi: 10.1111/jnu.13026. Epub 2024 Sep 18. J Nurs Scholarsh. 2025. PMID: 39294553 Free PMC article.
-
Integrated pulmonary index during procedural sedation and analgesia: A cluster-randomized trial.J Adv Nurs. 2025 Sep;81(9):5563-5572. doi: 10.1111/jan.16286. Epub 2024 Jun 26. J Adv Nurs. 2025. PMID: 38924169 Free PMC article. Clinical Trial.
-
Predicting Readmission Charges Billed by Hospitals: Machine Learning Approach.JMIR Med Inform. 2022 Aug 30;10(8):e37578. doi: 10.2196/37578. JMIR Med Inform. 2022. PMID: 35896038 Free PMC article.
-
Deep learning classification of capnography waveforms: secondary analysis of the PRODIGY study.J Clin Monit Comput. 2023 Oct;37(5):1327-1339. doi: 10.1007/s10877-023-01028-y. Epub 2023 May 13. J Clin Monit Comput. 2023. PMID: 37178234
References
-
- Lewandowska K, Weisbrot M, Cieloszyk A, Mędrzycka-Dąbrowska W, Krupa S, Ozga D. Impact of Alarm Fatigue on the Work of Nurses in an Intensive Care Environment-A Systematic Review. Int J Environ Res Public Health. 2020 Nov 13;17(22):8409. doi: 10.3390/ijerph17228409. https://www.mdpi.com/resolver?pii=ijerph17228409 ijerph17228409 - DOI - PMC - PubMed
-
- Apfelbaum J, Gross J, Connis R, Arnold D, Coté C, Dutton R, Tung A. Practice Guidelines for Moderate Procedural Sedation and Analgesia 2018: A Report by the American Society of Anesthesiologists Task Force on Moderate Procedural Sedation and Analgesia, the American Association of Oral and Maxillofacial Surgeons, American College of Radiology, American Dental Association, American Society of Dentist Anesthesiologists, and Society of Interventional Radiology. Anesthesiology. 2018 Mar;128(3):437–479. doi: 10.1097/ALN.0000000000002043. https://pubs.asahq.org/anesthesiology/article-lookup/doi/10.1097/ALN.000... - DOI - DOI - PubMed
-
- Hinkelbein J, Lamperti M, Akeson J, Santos J, Costa J, De Robertis Edoardo, Longrois D, Novak-Jankovic V, Petrini F, Struys Michel M R F, Veyckemans Francis, Fuchs-Buder Thomas, Fitzgerald Robert. European Society of Anaesthesiology and European Board of Anaesthesiology guidelines for procedural sedation and analgesia in adults. Eur J Anaesthesiol. 2018 Jan;35(1):6–24. doi: 10.1097/EJA.0000000000000683. - DOI - PubMed
-
- Dobson G, Chong MA, Chow L, Flexman A, Hurdle H, Kurrek M, Laflamme C, Perrault M, Sparrow K, Stacey S, Swart PA, Wong M. Procedural sedation: a position paper of the Canadian Anesthesiologists' Society. Can J Anaesth. 2018 Dec 27;65(12):1372–1384. doi: 10.1007/s12630-018-1230-z.10.1007/s12630-018-1230-z - DOI - PubMed
LinkOut - more resources
Full Text Sources
