

Eosinophilic Esophagitis: A Review
- PMID: 34609446
- PMCID: PMC9045493
- DOI: 10.1001/jama.2021.14920
Eosinophilic Esophagitis: A Review
Abstract
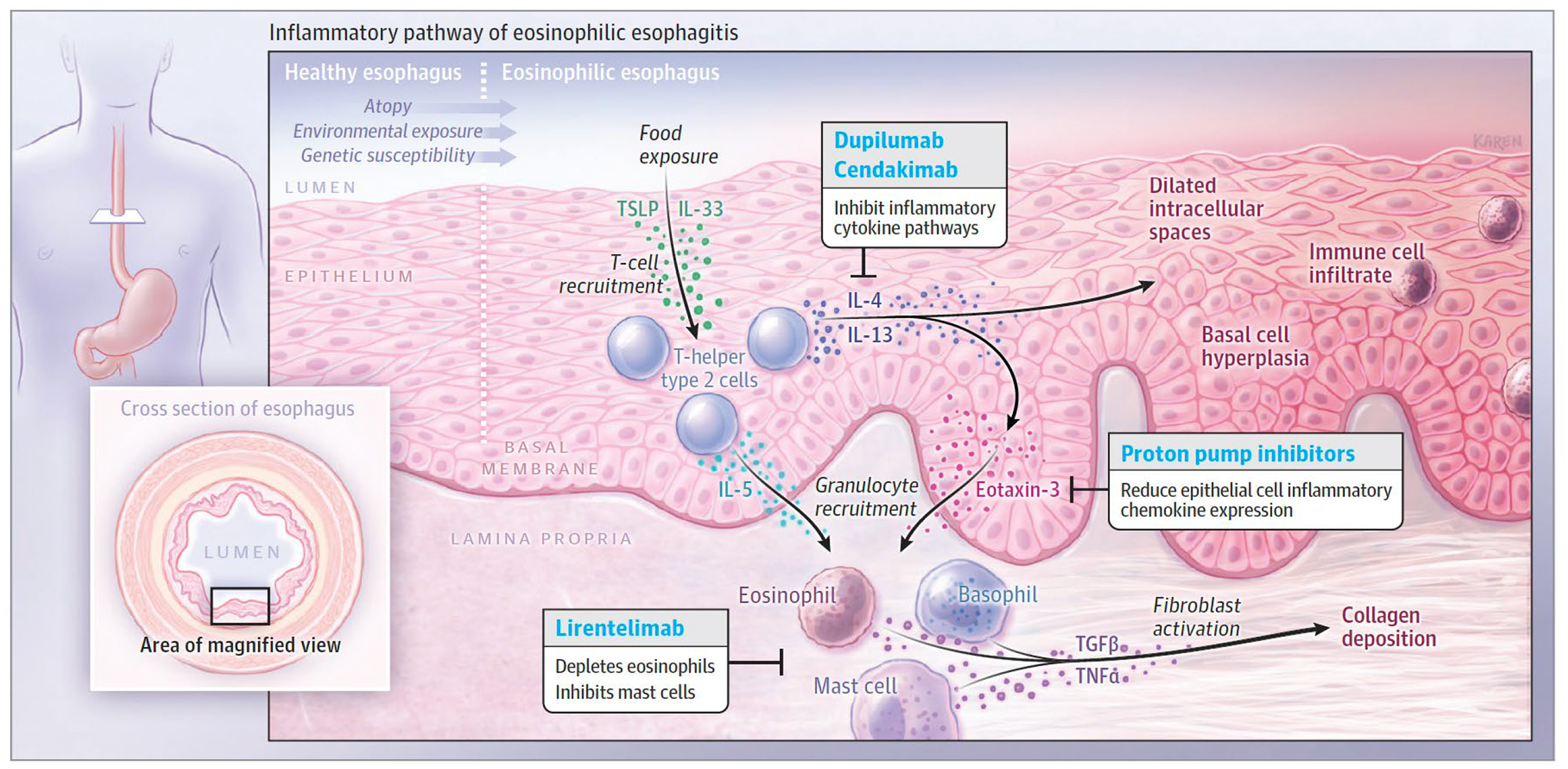
Importance: Eosinophilic esophagitis (EoE) is a chronic immune-mediated inflammatory disease of the esophagus that affects an estimated 34.4/100 000 people in Europe and North America. EoE affects both children and adults, and causes dysphagia, food impaction of the esophagus, and esophageal strictures.
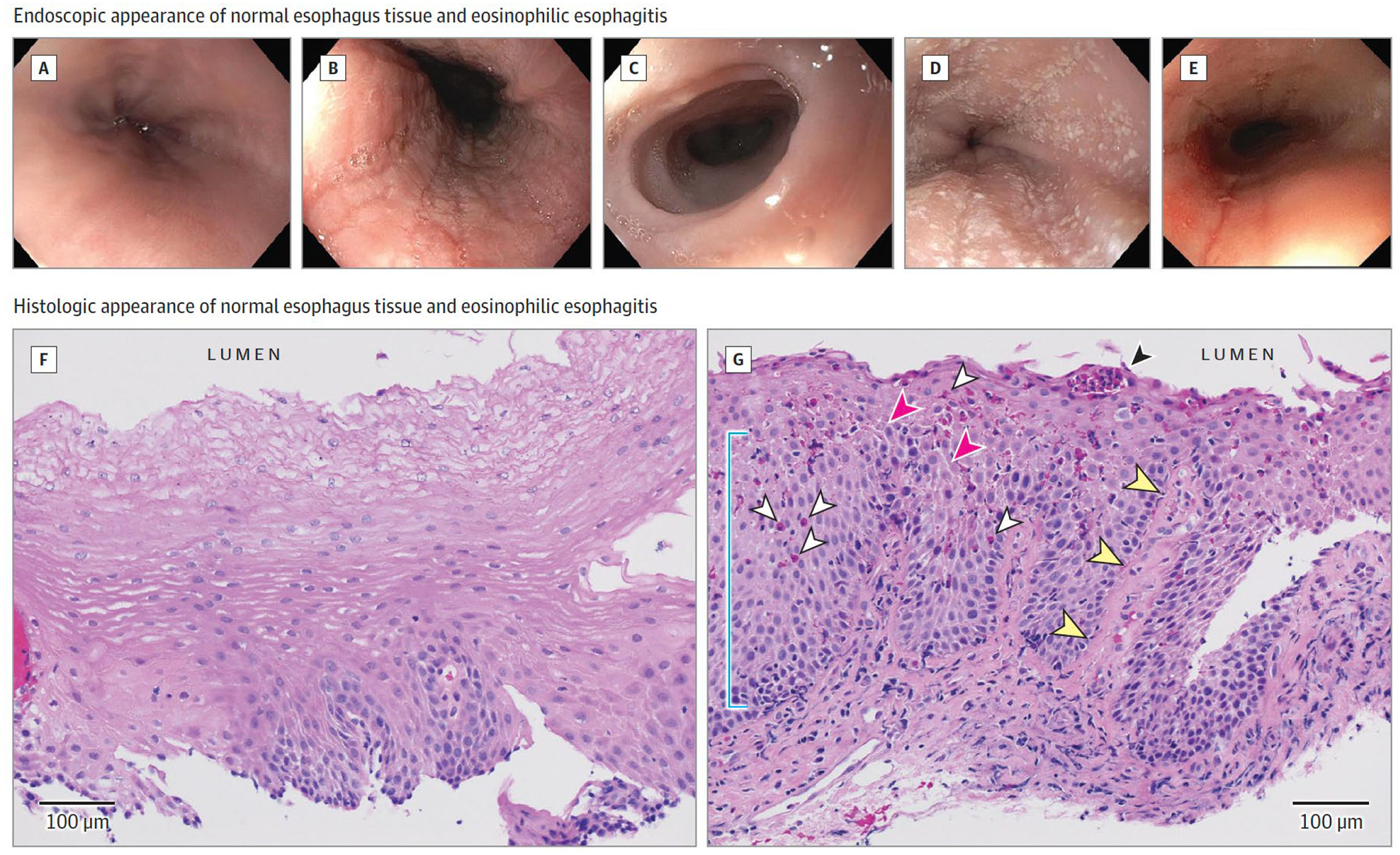
Observations: EoE is defined by symptoms of esophageal dysfunction, such as vomiting, dysphagia, or feeding difficulties, in a patient with an esophageal biopsy demonstrating at least 15 eosinophils per high-power field in the absence of other conditions associated with esophageal eosinophilia such as gastroesophageal reflux disease or achalasia. Genetic factors and environmental factors, such as exposure to antibiotics early in life, are associated with EoE. Current therapies include proton pump inhibitors; topical steroid preparations, such as fluticasone and budesonide; dietary therapy with amino acid formula or empirical food elimination; and endoscopic dilation. In a systematic review of observational studies that included 1051 patients with EoE, proton pump inhibitor therapy was associated with a histologic response, defined as less than 15 eosinophils per high-power field on endoscopic biopsy, in 41.7% of patients, while placebo was associated with a 13.3% response rate. In a systematic review of 8 randomized trials of 437 patients with EoE, topical corticosteroid treatment was associated with histologic remission in 64.9% of patients compared with 13.3% for placebo. Patients with esophageal narrowing may require dilation. Objective assessment of therapeutic response typically requires endoscopy with biopsy.
Conclusions and relevance: EoE has a prevalence of approximately 34.4/100 000 worldwide. Treatments consist of proton pump inhibitors, topical steroids, elemental diet, and empirical food elimination, with esophageal dilation reserved for patients with symptomatic esophageal narrowing.
Figures
References
-
- Navarro P, Arias Á, Arias-González L, Laserna-Mendieta EJ, Ruiz-Ponce M, Lucendo AJ. Systematic review with meta-analysis: the growing incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Alimentary Pharmacology and Therapeutics. 2019;49(9):1116–1125. doi:10.1111/apt.15231 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
