

Trends in Cardiovascular Risk Factors in US Adults by Race and Ethnicity and Socioeconomic Status, 1999-2018
- PMID: 34609450
- PMCID: PMC8493438
- DOI: 10.1001/jama.2021.15187
Trends in Cardiovascular Risk Factors in US Adults by Race and Ethnicity and Socioeconomic Status, 1999-2018
Abstract
Importance: After decades of decline, the US cardiovascular disease mortality rate flattened after 2010, and racial and ethnic differences in cardiovascular disease mortality persisted.
Objective: To examine 20-year trends in cardiovascular risk factors in the US population by race and ethnicity and by socioeconomic status.
Design, setting, and participants: A total of 50 571 participants aged 20 years or older from the 1999-2018 National Health and Nutrition Examination Surveys, a series of cross-sectional surveys in nationally representative samples of the US population, were included.
Exposures: Calendar year, race and ethnicity, education, and family income.
Main outcomes and measures: Age- and sex-adjusted means or proportions of cardiovascular risk factors and estimated 10-year risk of atherosclerotic cardiovascular disease were calculated for each of 10 two-year cycles.
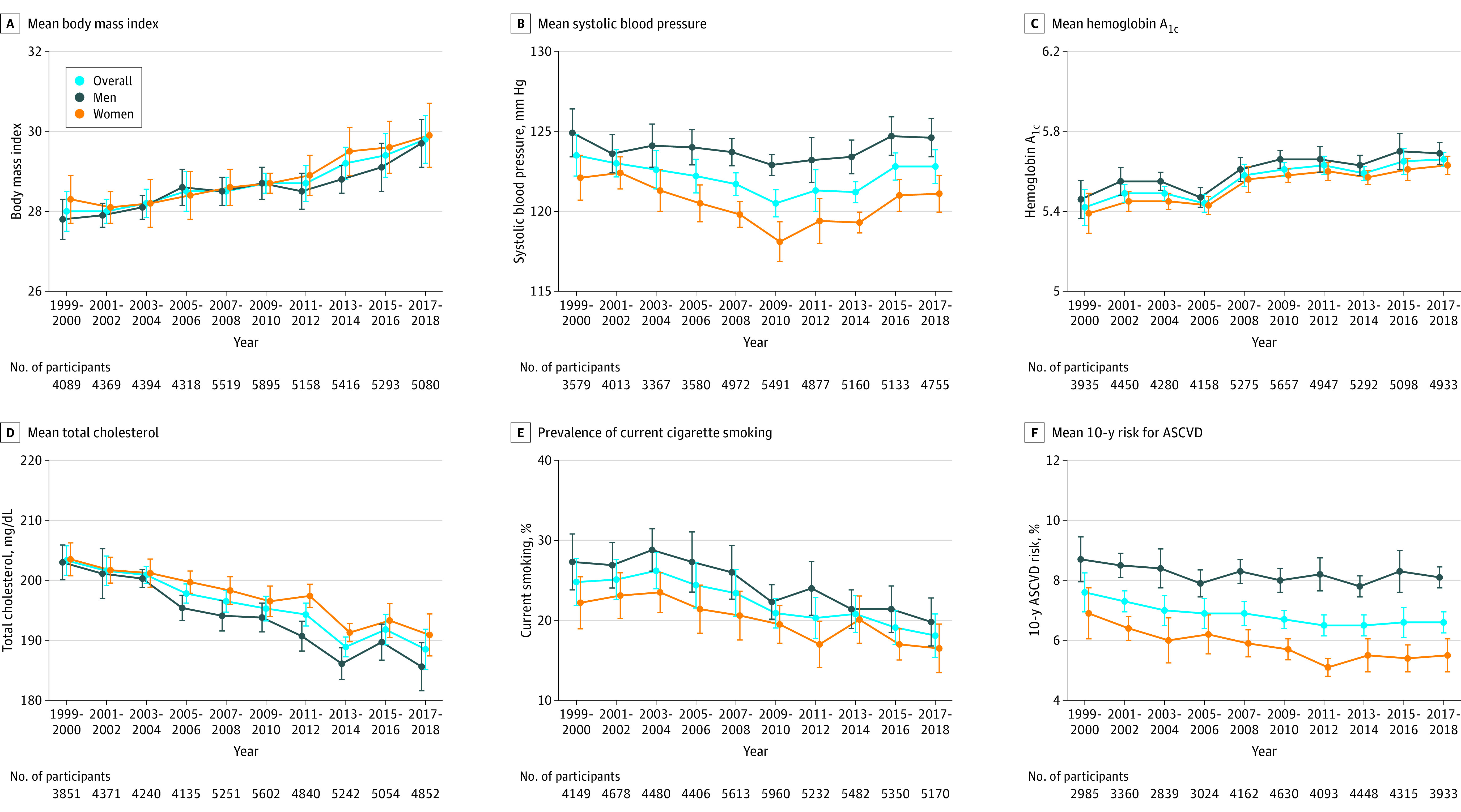
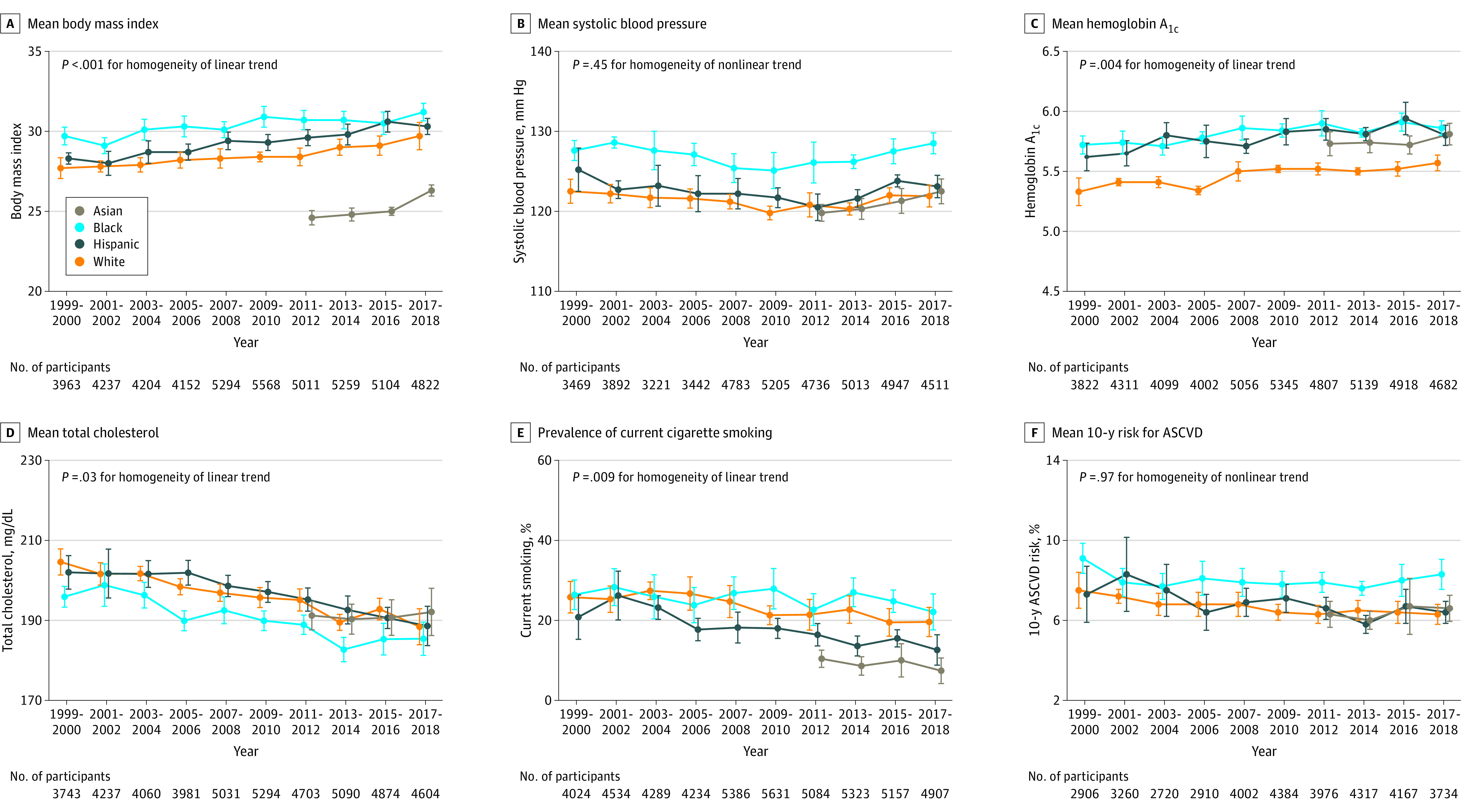
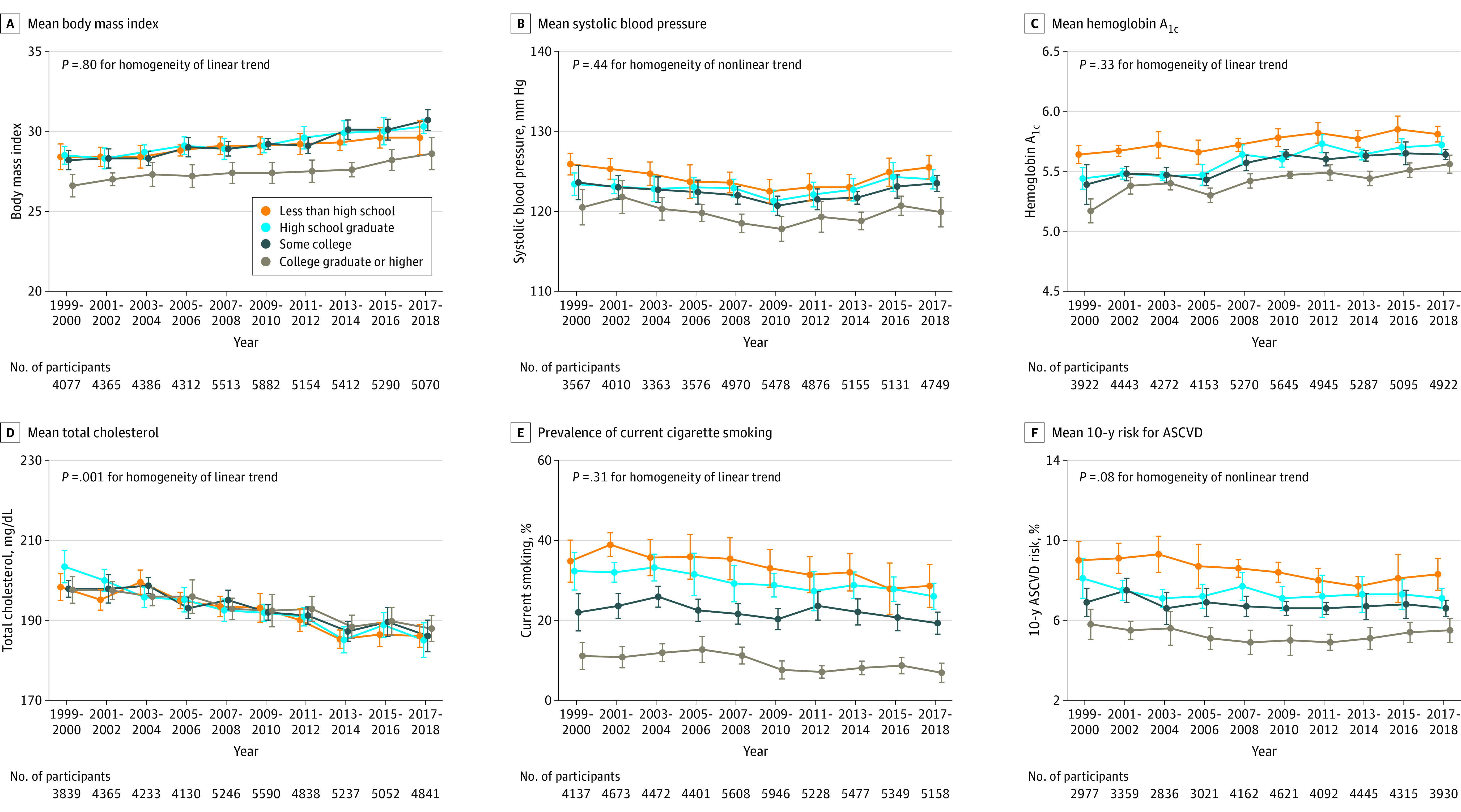
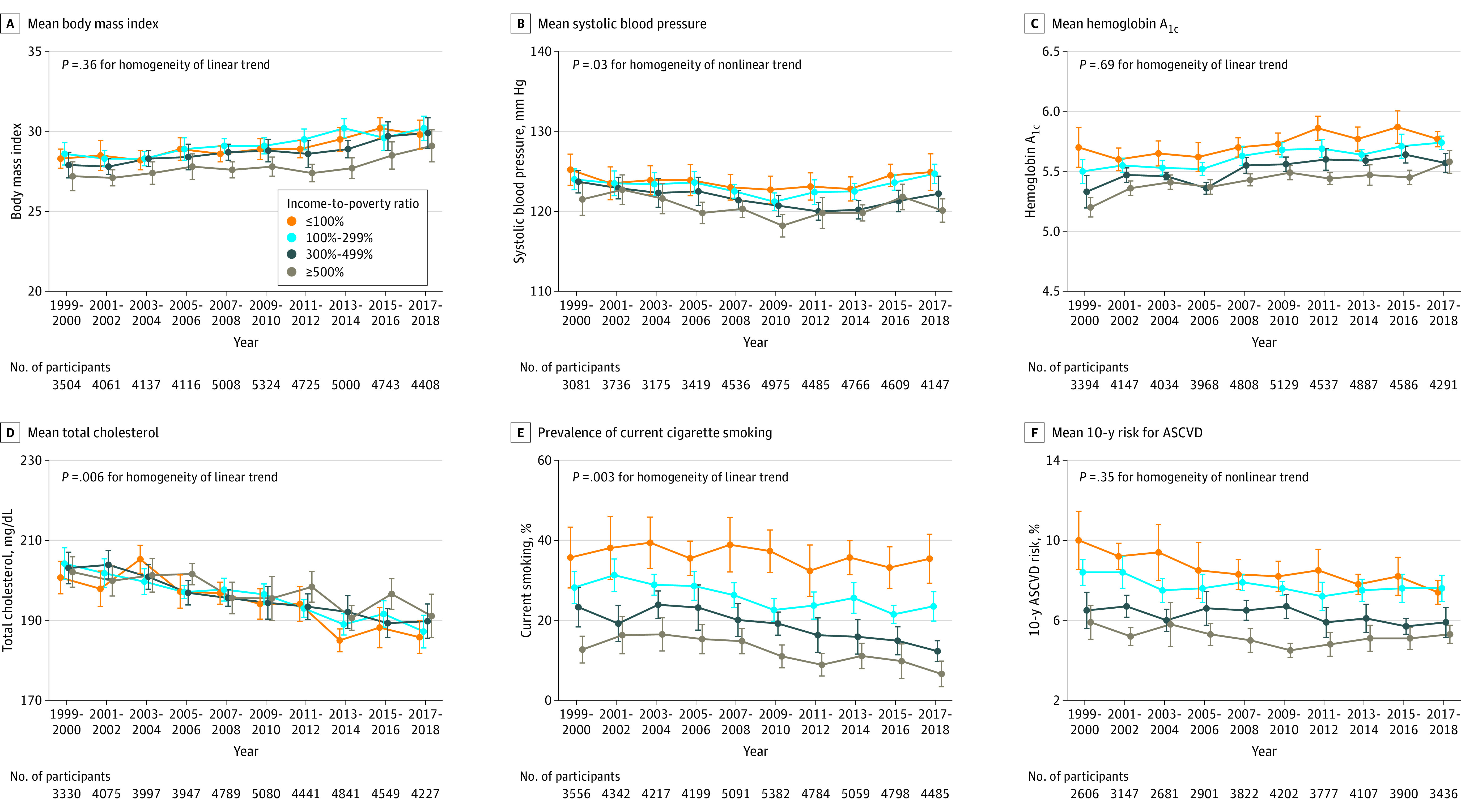
Results: The mean age of participants ranged from 49.0 to 51.8 years and the proportion of women from 48.2% to 51.3% in the surveys. From 1999-2000 to 2017-2018, age- and sex-adjusted mean body mass index increased from 28.0 (95% CI, 27.5-28.5) to 29.8 (95% CI, 29.2-30.4); mean hemoglobin A1c increased from 5.4% (95% CI, 5.3%-5.5%) to 5.7% (95% CI, 5.6%-5.7%) (both P < .001 for linear trends). Mean serum total cholesterol decreased from 203.3 mg/dL (95% CI, 200.9-205.8 mg/dL) to 188.5 mg/dL (95% CI, 185.2-191.9 mg/dL); prevalence of smoking decreased from 24.8% (95% CI, 21.8%-27.7%) to 18.1% (95% CI, 15.4%-20.8%) (both P < .001 for linear trends). Mean systolic blood pressure decreased from 123.5 mm Hg (95% CI, 122.2-124.8 mm Hg) in 1999-2000 to 120.5 mm Hg (95% CI, 119.6-121.3 mm Hg) in 2009-2010, then increased to 122.8 mm Hg (95% CI, 121.7-123.8 mm Hg) in 2017-2018 (P < .001 for nonlinear trend). Age- and sex-adjusted 10-year atherosclerotic cardiovascular disease risk decreased from 7.6% (95% CI, 6.9%-8.2%) in 1999-2000 to 6.5% (95% CI, 6.1%-6.8%) in 2011-2012, then did not significantly change. Age- and sex-adjusted body mass index, systolic blood pressure, and hemoglobin A1c were consistently higher, while total cholesterol was lower in non-Hispanic Black participants compared with non-Hispanic White participants (all P < .001 for group differences). Individuals with college or higher education or high family income had consistently lower levels of cardiovascular risk factors. The mean age- and sex-adjusted 10-year risk of atherosclerotic cardiovascular disease was significantly higher in non-Hispanic Black participants compared with non-Hispanic White participants (difference, 1.4% [95% CI, 1.0%-1.7%] in 1999-2008 and 2.0% [95% CI, 1.7%-2.4%] in 2009-2018]). This difference was attenuated (-0.3% [95% CI, -0.6% to 0.1%] in 1999-2008 and 0.7% [95% CI, 0.3%-1.0%] in 2009-2018) after further adjusting for education, income, home ownership, employment, health insurance, and access to health care.
Conclusions and relevance: In this serial cross-sectional survey study that estimated US trends in cardiovascular risk factors from 1999 through 2018, differences in cardiovascular risk factors persisted between Black and White participants; the difference may have been moderated by social determinants of health.
Conflict of interest statement
Figures
References
-
- Virani SS, Alonso A, Aparicio HJ, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e254-e743. doi:10.1161/CIR.0000000000000950 - DOI - PubMed
-
- Murphy SL, Xu J, Kochanek KD, Arias E, Tejada-Vera B. Deaths: final data for 2018. Natl Vital Stat Rep. 2021;69(13):1-83. - PubMed
