US Emergency Department Visits Attributed to Medication Harms, 2017-2019
- PMID: 34609453
- PMCID: PMC8493432
- DOI: 10.1001/jama.2021.13844
US Emergency Department Visits Attributed to Medication Harms, 2017-2019
Abstract
Importance: Assessing the scope of acute medication harms to patients should include both therapeutic and nontherapeutic medication use.
Objective: To describe the characteristics of emergency department (ED) visits for acute harms from both therapeutic and nontherapeutic medication use in the US.
Design, setting, and participants: Active, nationally representative, public health surveillance based on patient visits to 60 EDs in the US participating in the National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance Project from 2017 through 2019.
Exposures: Medications implicated in ED visits, with visits attributed to medication harms (adverse events) based on the clinicians' diagnoses and supporting data documented in the medical record.
Main outcomes and measures: Nationally weighted estimates of ED visits and subsequent hospitalizations for medication harms.
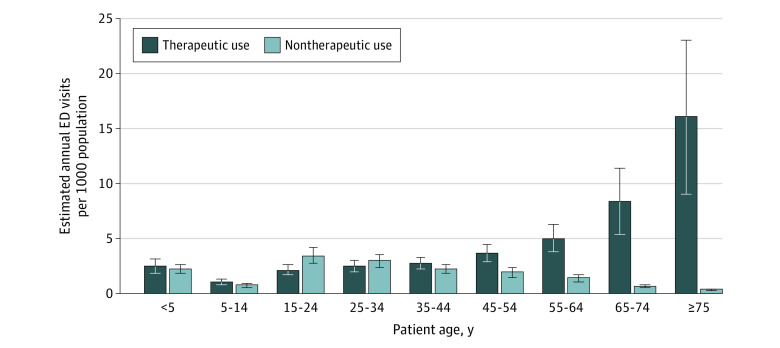
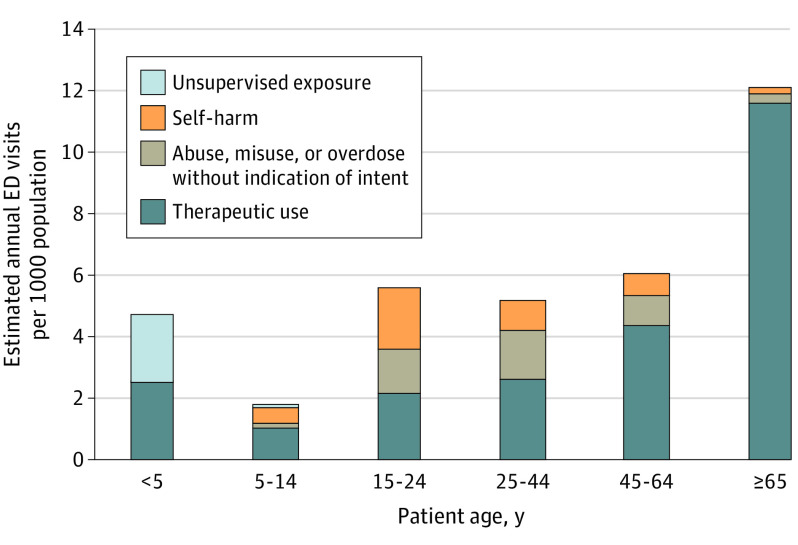
Results: Based on 96 925 cases (mean patient age, 49 years; 55% female), there were an estimated 6.1 (95% CI, 4.8-7.5) ED visits for medication harms per 1000 population annually and 38.6% (95% CI, 35.2%-41.9%) resulted in hospitalization. Population rates of ED visits for medication harms were higher for patients aged 65 years or older than for those younger than 65 years (12.1 vs 5.0 [95% CI, 7.4-16.8 vs 4.1-5.8] per 1000 population). Overall, an estimated 69.1% (95% CI, 63.6%-74.7%) of ED visits for medication harms involved therapeutic medication use, but among patients younger than 45 years, an estimated 52.5% (95% CI, 48.1%-56.8%) of visits for medication harms involved nontherapeutic use. The proportions of ED visits for medication harms involving therapeutic use were lowest for barbiturates (6.3%), benzodiazepines (11.1%), nonopioid analgesics (15.7%), and antihistamines (21.8%). By age group, the most frequent medication types and intents of use associated with ED visits for medication harms were therapeutic use of anticoagulants (4.5 [95% CI, 2.3-6.7] per 1000 population) and diabetes agents (1.8 [95% CI, 1.3-2.3] per 1000 population) for patients aged 65 years and older; therapeutic use of diabetes agents (0.8 [95% CI, 0.5-1.0] per 1000 population) for patients aged 45 to 64 years; nontherapeutic use of benzodiazepines (1.0 [95% CI, 0.7-1.3] per 1000 population) for patients aged 25 to 44 years; and unsupervised medication exposures (2.2 [95% CI, 1.8-2.7] per 1000 population) and therapeutic use of antibiotics (1.4 [95% CI, 1.0-1.8] per 1000 population) for children younger than 5 years.
Conclusions and relevance: According to data from 60 nationally representative US emergency departments, visits attributed to medication harms in 2017-2019 were frequent, with variation in products and intent of use by age.
Conflict of interest statement
Figures