

Cardiovascular consequences of viral infections: from COVID to other viral diseases
- PMID: 34609508
- PMCID: PMC8500164
- DOI: 10.1093/cvr/cvab315
Cardiovascular consequences of viral infections: from COVID to other viral diseases
Abstract
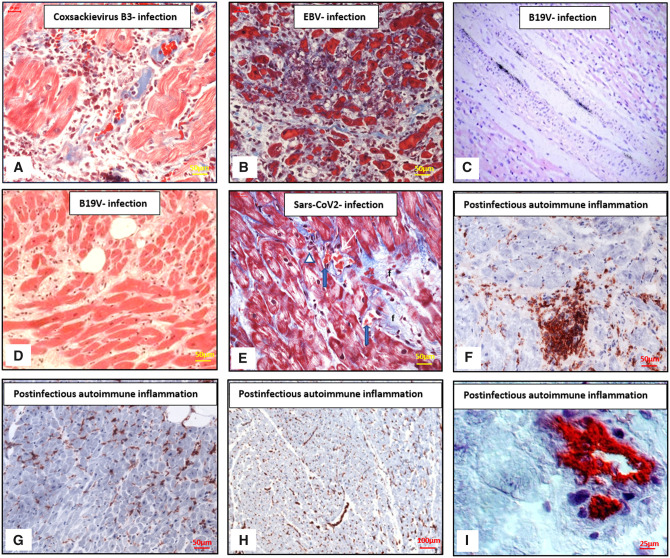
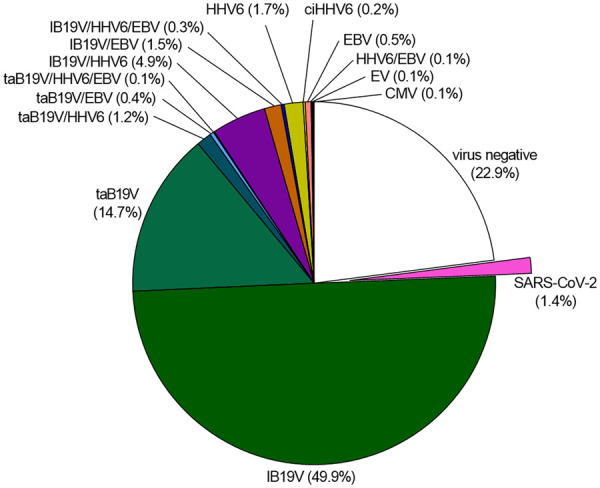
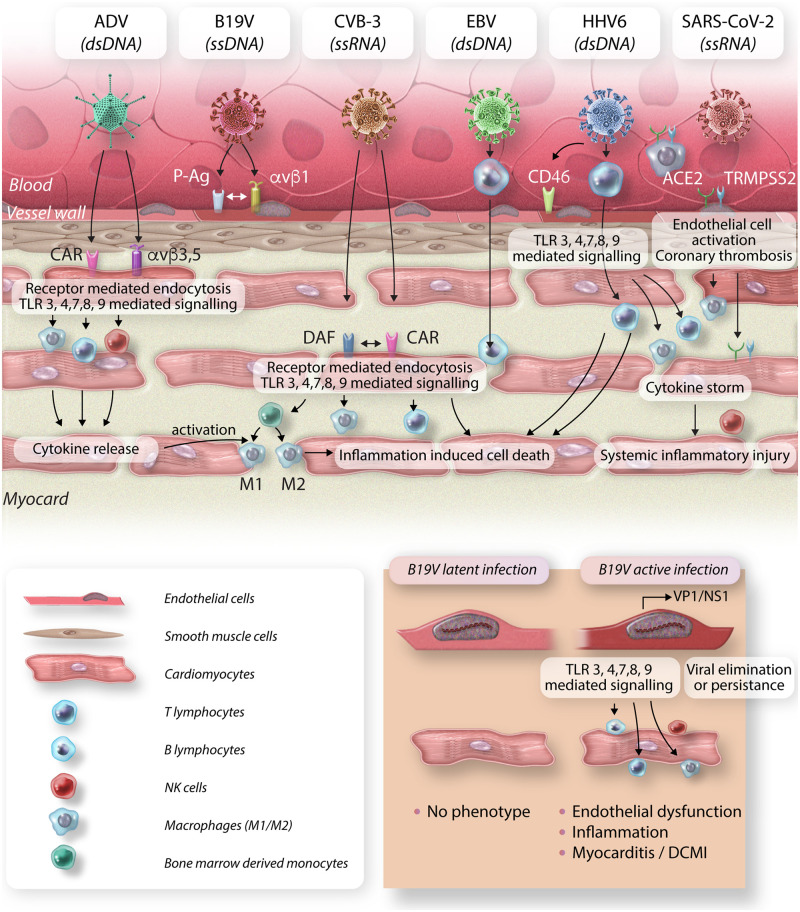
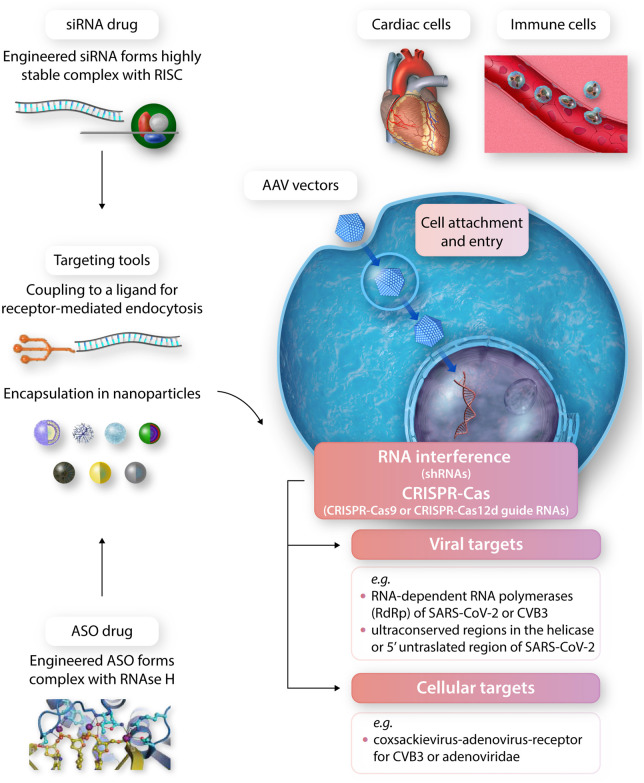
Infection of the heart muscle with cardiotropic viruses is one of the major aetiologies of myocarditis and acute and chronic inflammatory cardiomyopathy (DCMi). However, viral myocarditis and subsequent dilated cardiomyopathy is still a challenging disease to diagnose and to treat and is therefore a significant public health issue globally. Advances in clinical examination and thorough molecular genetic analysis of intramyocardial viruses and their activation status have incrementally improved our understanding of molecular pathogenesis and pathophysiology of viral infections of the heart muscle. To date, several cardiotropic viruses have been implicated as causes of myocarditis and DCMi. These include, among others, classical cardiotropic enteroviruses (Coxsackieviruses B), the most commonly detected parvovirus B19, and human herpes virus 6. A newcomer is the respiratory virus that has triggered the worst pandemic in a century, SARS-CoV-2, whose involvement and impact in viral cardiovascular disease is under scrutiny. Despite extensive research into the pathomechanisms of viral infections of the cardiovascular system, our knowledge regarding their treatment and management is still incomplete. Accordingly, in this review, we aim to explore and summarize the current knowledge and available evidence on viral infections of the heart. We focus on diagnostics, clinical relevance and cardiovascular consequences, pathophysiology, and current and novel treatment strategies.
Keywords: Advanced diagnostics; Inflammatory cardiomyopathy; Myocarditis; Treatment strategies; Viral infections.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Serological and Molecular Biological Studies of Parvovirus B19, Coxsackie B Viruses, and Adenoviruses as Potential Cardiotropic Viruses in Bulgaria.Folia Med (Plovdiv). 2016 Dec 1;58(4):250-256. doi: 10.1515/folmed-2016-0036. Folia Med (Plovdiv). 2016. PMID: 28068282
-
Prevalence of the parvovirus B19 genome in endomyocardial biopsy specimens.Hum Pathol. 2003 May;34(5):497-503. doi: 10.1016/s0046-8177(03)00078-9. Hum Pathol. 2003. PMID: 12792925
-
Fatal parvovirus B19 myocarditis in children and possible dysimmune mechanism.Pediatr Infect Dis J. 2012 Apr;31(4):418-21. doi: 10.1097/INF.0b013e3182425786. Pediatr Infect Dis J. 2012. PMID: 22173134
-
Myocarditis and inflammatory cardiomyopathy: current evidence and future directions.Nat Rev Cardiol. 2021 Mar;18(3):169-193. doi: 10.1038/s41569-020-00435-x. Epub 2020 Oct 12. Nat Rev Cardiol. 2021. PMID: 33046850 Free PMC article. Review.
-
Pathophysiology and aetiological diagnosis of inflammatory myocardial diseases with a special focus on parvovirus B19.J Vet Med B Infect Dis Vet Public Health. 2005 Sep-Oct;52(7-8):344-7. doi: 10.1111/j.1439-0450.2005.00873.x. J Vet Med B Infect Dis Vet Public Health. 2005. PMID: 16316398 Review.
Cited by
-
Giant cell myocarditis after first dose of BNT162b2 - a case report.Eur J Heart Fail. 2022 Jul;24(7):1319-1322. doi: 10.1002/ejhf.2590. Epub 2022 Jul 11. Eur J Heart Fail. 2022. PMID: 35733299 Free PMC article.
-
Skeletal Muscle and COVID-19: The Potential Involvement of Bioactive Sphingolipids.Biomedicines. 2022 May 4;10(5):1068. doi: 10.3390/biomedicines10051068. Biomedicines. 2022. PMID: 35625805 Free PMC article. Review.
-
Impact of first and second/third wave of COVID-19 pandemic on post-acute cardiovascular outcomes in Lombardy.Front Cardiovasc Med. 2023 Sep 12;10:1244002. doi: 10.3389/fcvm.2023.1244002. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37781303 Free PMC article.
-
Cardiovascular manifestations secondary to COVID-19: A narrative review.Respir Med Res. 2022 May;81:100904. doi: 10.1016/j.resmer.2022.100904. Epub 2022 May 4. Respir Med Res. 2022. PMID: 35525097 Free PMC article. Review.
-
Editorial: Viral hypothesis in cardiac arrhythmias.Front Cardiovasc Med. 2022 Dec 9;9:1067501. doi: 10.3389/fcvm.2022.1067501. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36568549 Free PMC article. No abstract available.
References
-
- Caforio ALP, Pankuweit S, Arbustini E, Basso C, Gimeno-Blanes J, Felix SB, Fu M, Heliö T, Heymans S, Jahns R, Klingel K, Linhart A, Maisch B, McKenna W, Mogensen J, Pinto YM, Ristic A, Schultheiss H-P, Seggewiss H, Tavazzi L, Thiene G, Yilmaz A, Charron P, Elliott PM; European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013;34:2636–2648. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
