

Comprehensive review of the recent advances in devices for endovascular treatment of complex brain aneurysms
- PMID: 34609898
- PMCID: PMC8722252
- DOI: 10.1259/bjr.20210538
Comprehensive review of the recent advances in devices for endovascular treatment of complex brain aneurysms
Abstract
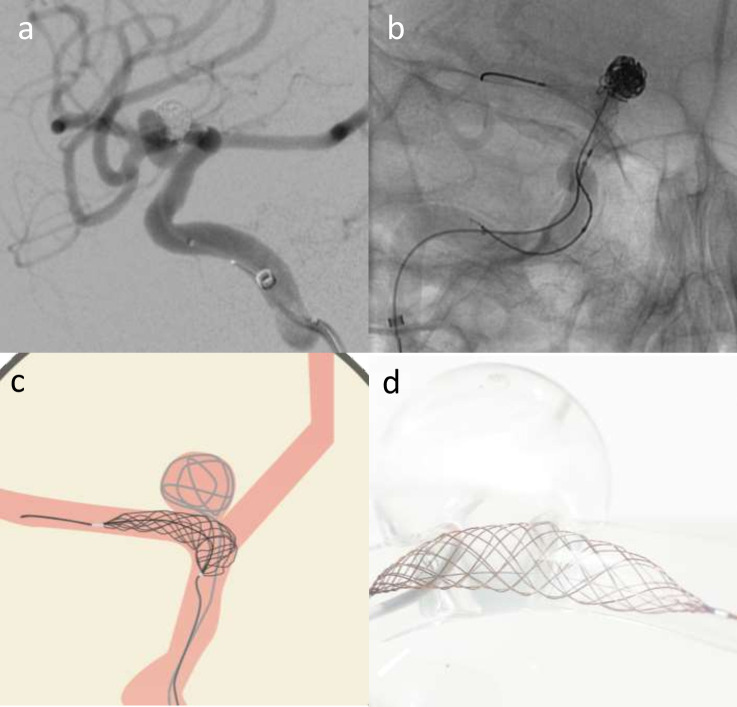
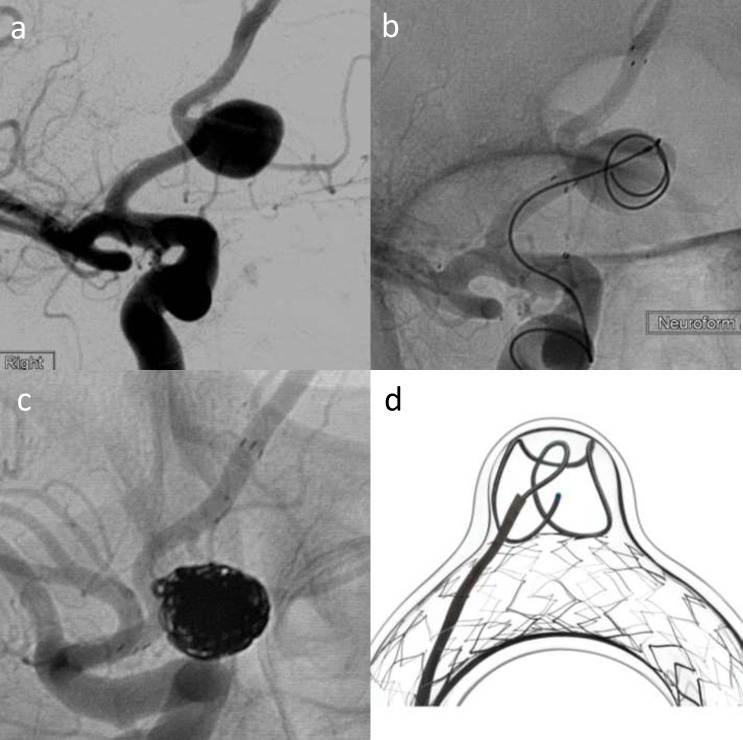
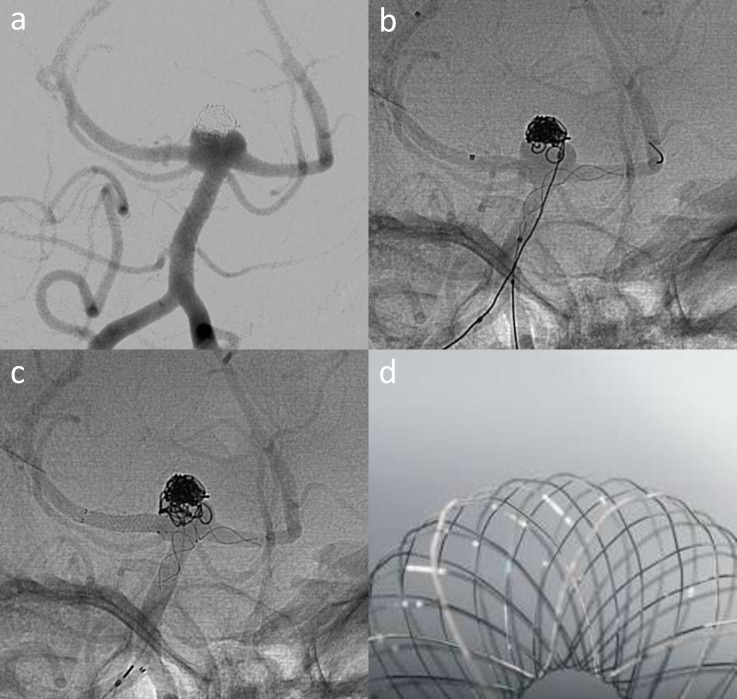
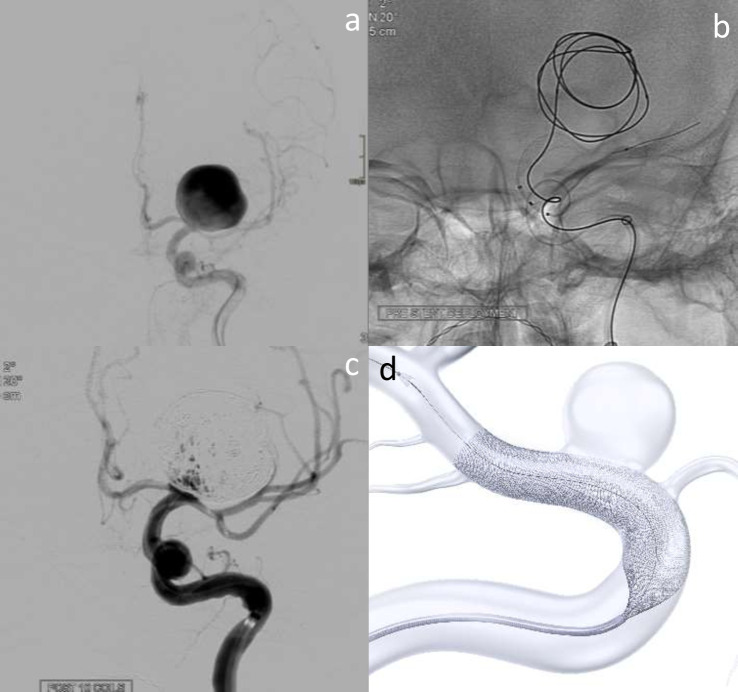
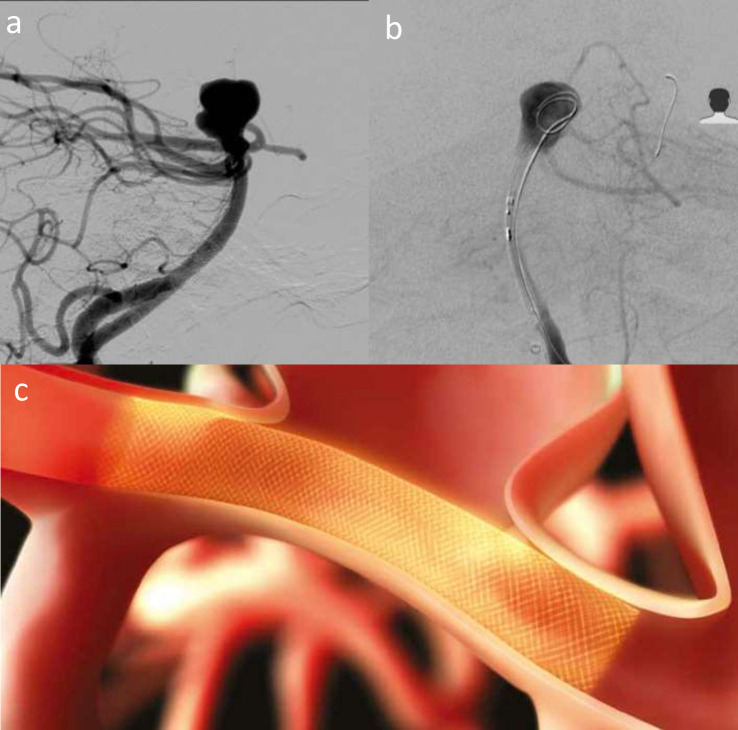
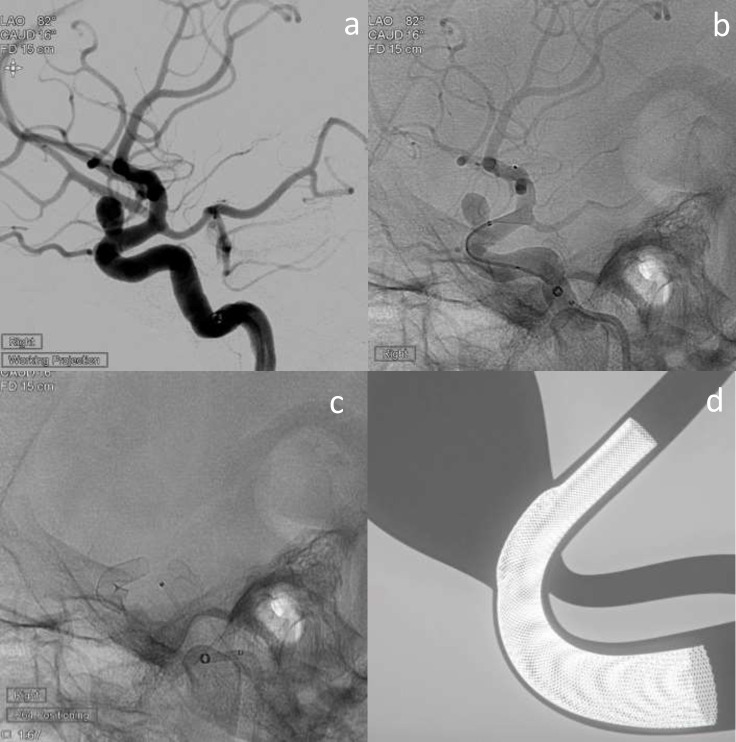
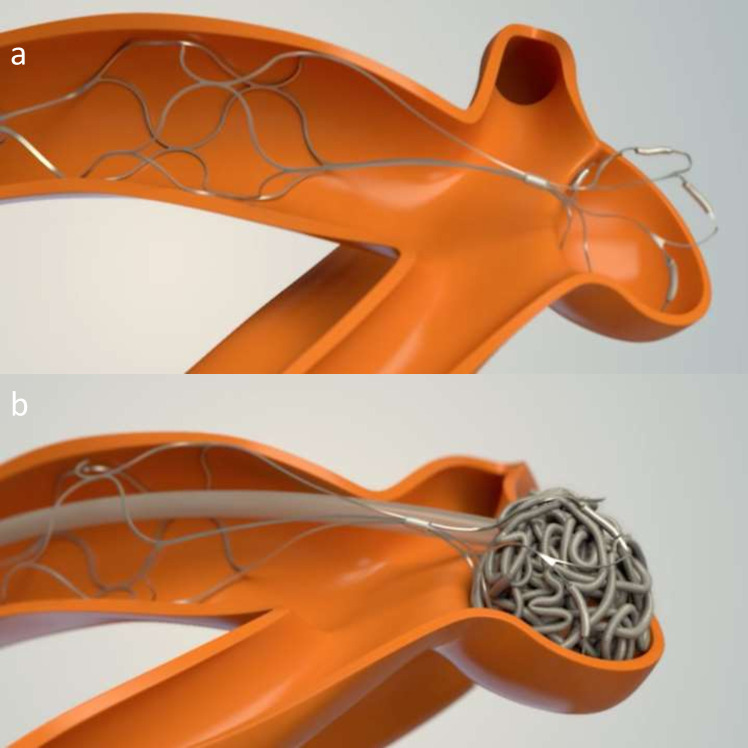
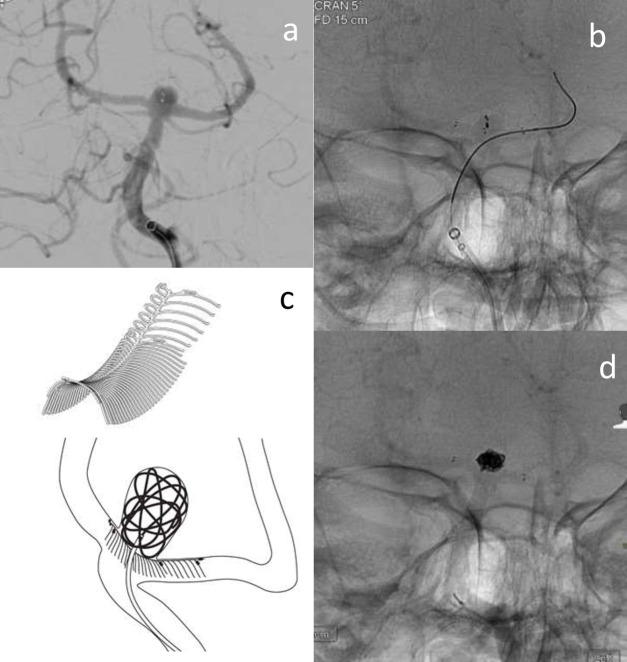
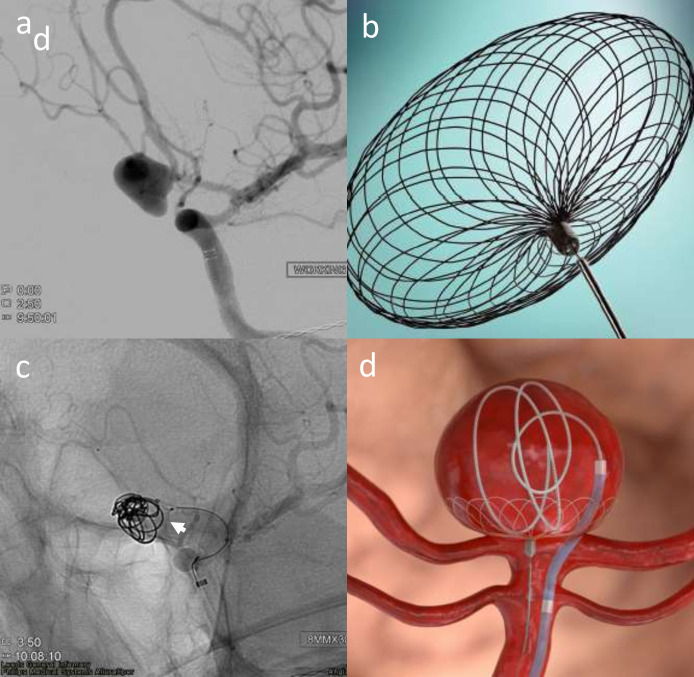
The International Subarachnoid Aneurysm Trial (ISAT) showed superiority for endovascular treatment of ruptured aneurysms and technology has since moved on rapidly. Many approaches and technology now exist for the endovascular management of ruptured and unruptured intracranial aneurysms, which reflects their varied nature - there is no one-size-fits-all technique. We aim to provide an overview of the various classes of device and the major developments over the past decade. Coiling is the oldest of the technology and continues to demonstrate high levels of occlusion and acceptable risks, making it the default treatment choice, particularly in the acutely ruptured aneurysm setting. Advances on coiling include the use of adjuncts such as balloons, stents and fully retrievable temporary neck-bridging devices, which have facilitated the treatment of more complex aneurysms. Flow divertors have also revolutionised complex aneurysm treatment with small added risk in acute aneurysm treatment and seek to remodel the aneurysm-vessel interface without accessing the aneurysm sac. The latest development and most promising avenue appears to be intrasaccular flow disrupting devices like WEB, Contour and Neqstent that provide excellent opportunities to treat wide neck complex aneurysm with minimal mortality and morbidity and good occlusion rates and may in future replace a significant number of stent-assisted coiling too.
Figures

References
-
- Molyneux AJ, Kerr RSC, Yu L-M, Clarke M, Sneade M, Yarnold JA, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005; 366: 809–17. doi: 10.1016/S0140-6736(05)67214-5 - DOI - PubMed
-
- Pierot L, Barbe C, Herbreteau D, Gauvrit J-Y, Januel A-C, Bala F, et al. Rebleeding and bleeding in the year following intracranial aneurysm coiling: analysis of a large prospective multicenter cohort of 1140 patients-Analysis of recanalization after endovascular treatment of intracranial aneurysm (ARETA) study. J Neurointerv Surg 2020; 12: 1219–25. doi: 10.1136/neurintsurg-2020-015971 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
