

MRI-directed biopsy for primary detection of prostate cancer in a population of 223 men: MRI In-Bore vs MRI-transrectal ultrasound fusion-targeted techniques
- PMID: 34609900
- PMCID: PMC8978234
- DOI: 10.1259/bjr.20210528
MRI-directed biopsy for primary detection of prostate cancer in a population of 223 men: MRI In-Bore vs MRI-transrectal ultrasound fusion-targeted techniques
Abstract
Objectives: To compare the detection rates of overall prostate cancer (PCa) and clinically significant PCa (csPCa) and the median percentage of cancer per biopsy core between MRI-guided In-bore and MRI-TRUS fusion-targeted biopsy (TBx).
Methods: In this retrospective study, 223 patients who underwent prostate multiparametric MRI (mpMRI) and subsequent MR-directed biopsy were included. For PCa and csPCa detection rate (DR), contingency tables were tested via the Pearson's chi-squared to explore the variance of the outcome distribution. The percentage of cancer per biopsy core was tested with a two-tailed Mann-Withney test.
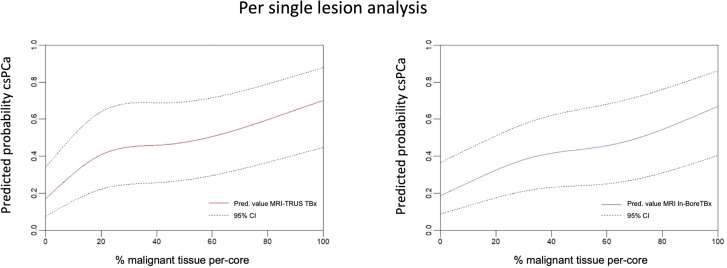
Results: One hundred and seventeen and 106 patients underwent MRI-TRUS fusion or MRI In-bore TBx, respectively. 402 MRI biopsy targets were identified, of which 206 (51.2%) were biopsied with the MRI-TRUS TBx and 196 (48.8%) with the MRI In-bore TBx technique. Per-patient PCa and csPCa detection rates were 140/223 (62.8%) and 97/223 (43.5%), respectively. PCa-DR was 73/117 (62.4%) and 67/106 (63.2%) for MRI-TRUS and MRI In-Bore TBx (p = 0.9), while csPCa detection rate reached 50/117 (42.7%) and 47/106 (44.3%), respectively (p = 0.81). The median per-patient percentage of malignant tissue within biopsy cores was 50% (IQR: 27-65%) for PCa and 60% (IQR: 35-68%) for csPCa, with a statistically significant difference between the techniques.
Conclusion: No statistically significant difference in the detection rate of MRI In-bore and MRI-TRUS fusion TBx was found. MRI In-bore TBx showed higher per-core percentage of malignant cells.
Advances in knowledge: MRI In-bore biopsy might impact risk stratification and patient management considering the higher per-core percentage of malignant cells, especially for patients eligible for active surveillance or focal therapy.
Figures
Similar articles
-
Prostate Cancer Risk Assessment in Biopsy-naïve Patients: The Rotterdam Prostate Cancer Risk Calculator in Multiparametric Magnetic Resonance Imaging-Transrectal Ultrasound (TRUS) Fusion Biopsy and Systematic TRUS Biopsy.Eur Urol Oncol. 2018 Jun;1(2):109-117. doi: 10.1016/j.euo.2018.02.010. Epub 2018 May 15. Eur Urol Oncol. 2018. PMID: 31100233
-
Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Multicenter Clinical Study.Eur Urol. 2019 Apr;75(4):570-578. doi: 10.1016/j.eururo.2018.11.023. Epub 2018 Nov 23. Eur Urol. 2019. PMID: 30477981
-
Comparison of Cancer Detection Rates Between TRUS-Guided Biopsy and MRI-Targeted Biopsy According to PSA Level in Biopsy-Naive Patients: A Propensity Score Matching Analysis.Clin Genitourin Cancer. 2019 Feb;17(1):e19-e25. doi: 10.1016/j.clgc.2018.09.007. Epub 2018 Sep 13. Clin Genitourin Cancer. 2019. PMID: 30415878
-
Elastic Versus Rigid Image Registration in Magnetic Resonance Imaging-transrectal Ultrasound Fusion Prostate Biopsy: A Systematic Review and Meta-analysis.Eur Urol Focus. 2018 Mar;4(2):219-227. doi: 10.1016/j.euf.2016.07.003. Epub 2016 Jul 29. Eur Urol Focus. 2018. PMID: 28753777
-
Follow-up of negative MRI-targeted prostate biopsies: when are we missing cancer?World J Urol. 2019 Feb;37(2):235-241. doi: 10.1007/s00345-018-2337-0. Epub 2018 May 21. World J Urol. 2019. PMID: 29785491 Review.
Cited by
-
Imaging of clinically silent rectoprostatic hematoma in MRI guided in-bore prostate biopsy.Sci Rep. 2022 Feb 3;12(1):1840. doi: 10.1038/s41598-022-05909-1. Sci Rep. 2022. PMID: 35115642 Free PMC article.
-
Pathological Accuracy in Prostate Cancer: Single-Center Outcomes of 3 Different Magnetic Resonance Imaging-Targeted Biopsy Techniques and Random Systematic Biopsy.Turk J Urol. 2022 Sep;48(5):346-353. doi: 10.5152/tud.2022.22165. Turk J Urol. 2022. PMID: 36197141 Free PMC article.
-
TRUS-Guided Target Biopsy for a PI-RADS 3-5 Index Lesion to Reduce Gleason Score Underestimation: A Propensity Score Matching Analysis.Front Oncol. 2022 Jan 24;11:824204. doi: 10.3389/fonc.2021.824204. eCollection 2021. Front Oncol. 2022. PMID: 35141158 Free PMC article.
-
Innovations in prostate cancer: introductory editorial.Br J Radiol. 2022 Mar;95(1131):20229003. doi: 10.1259/bjr.20229003. Br J Radiol. 2022. PMID: 35179398 Free PMC article. No abstract available.
-
Concordance of MRI-Guided Fusion and Systematic 12-Core Prostate Biopsy for the Detection of Prostate Cancer.Front Oncol. 2022 May 27;12:899567. doi: 10.3389/fonc.2022.899567. eCollection 2022. Front Oncol. 2022. PMID: 35692776 Free PMC article.
References
-
- Mottet RCN, van den Bergh N, Brier E, Cornford P, De Santis M, Fanti S. EAU guidelines: prostate cancer. EAU guidelines. 978th-94th-92671st-04-2. ed; 2019.
-
- Faria R, Soares MO, Spackman E, Ahmed HU, Brown LC, Kaplan R, et al. . Optimising the diagnosis of prostate cancer in the era of multiparametric magnetic resonance imaging: a cost-effectiveness analysis based on the prostate MR imaging study (PROMIS). Eur Urol 2018; 73: 23–30. doi: 10.1016/j.eururo.2017.08.018 - DOI - PMC - PubMed
-
- Panebianco V, Valerio MC, Giuliani A, Pecoraro M, Ceravolo I, Barchetti G, et al. . Clinical utility of multiparametric magnetic resonance imaging as the first-line tool for men with high clinical suspicion of prostate cancer. Eur Urol Oncol 2018; 1: 208–14. doi: 10.1016/j.euo.2018.03.008 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
