

The Pre- and Postoperative Prevalence and Risk Factors of ASA Nonresponse in Vascular Surgery
- PMID: 34609920
- PMCID: PMC8642110
- DOI: 10.1177/10760296211044723
The Pre- and Postoperative Prevalence and Risk Factors of ASA Nonresponse in Vascular Surgery
Abstract
Background: An antiplatelet therapy with acetylsalicylic acid (ASA) is prescribed in the prevention of cardiovascular events, but around 24% of ASA takers are resistant to the treatment.
Aim: In this prospective, observational cohort study, we aimed to identify the prevalence and risk factors of ASA nonresponse in patients who underwent vascular surgery.
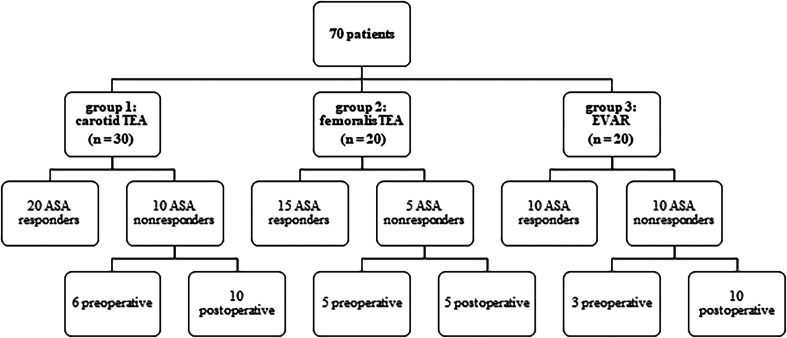
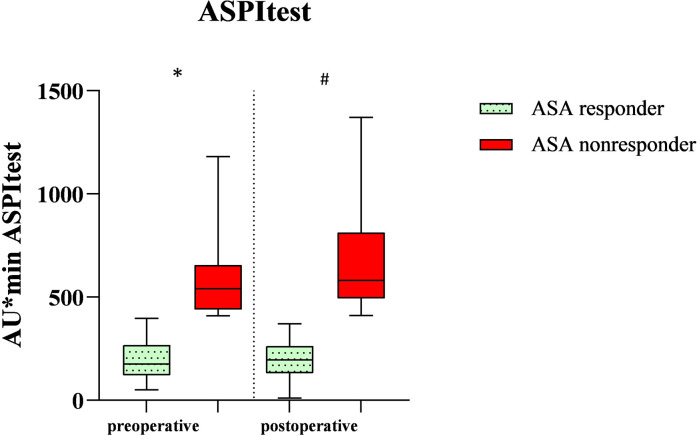
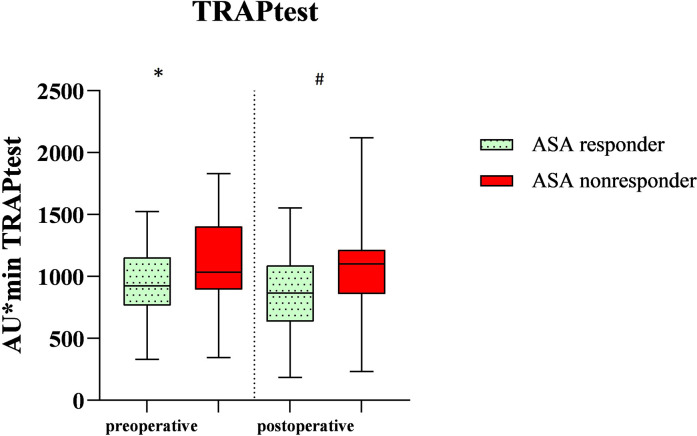
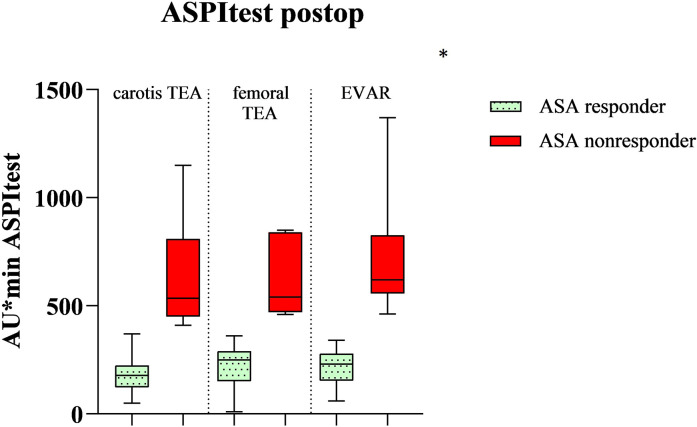
Methods: The study was conducted in the University hospital in Frankfurt am Main. In total, 70 patients were pre-treated with 100 mg of ASA per day and underwent either elective carotid thromboendarterectomy, femoral thromboendarterectomy or endovascular aneurysm repair of the abdominal aorta. The platelet function was measured on the first preoperative and the second or fourth postoperative day with the multiple electrode aggregometry by in-vitro stimulation with arachidonic acid (ASPItest) and thrombin receptor activating peptide 6 (TRAPtest). The primary end point was the in-vitro induced platelet aggregation in the ASPItest. If the ASPItest amounted ≥400 AU × min, the patients were categorized as ASA nonresponders.
Results: The total prevalence of ASA nonresponse in our study was 20% preoperatively and 35.7% postoperatively (p = 0.005). As significant predictors for ASA nonresponse, we demonstrated the area under the aggregation curve in the TRAPtest preoperatively (p = 0.04) and postoperatively (p = 0.02), and the two comorbidities arterial hypertension (P < .001; rho 0.44) and diabetes mellitus (p = 0.04; rho 0.39), which are already well known to be associated with ASA nonresponse.
Conclusion: In conclusion, data of the study indicate a high incidence of perioperative, laboratory ASA nonresponse in patients undergoing vascular surgery.
Keywords: ASA nonresponse; Multiplate Analyzer; platelet aggregation; vascular surgery.
Conflict of interest statement
Figures
References
-
- Assadian A, Lax J, Meixner-Loicht U, Hagmüller GW, Bayer PM, Hübl W. Aspirin resistance among long-term aspirin users after carotid endarterectomy and controls: flow cytometric measurement of aspirin-induced platelet inhibition. J Vasc Surg. 2007;45(6):1142-1147. discussion 1147. - PubMed
-
- Wong S, Appleberg M, Ward CM, Lewis DR. Aspirin resistance in cardiovascular disease: a review. European Journal of Vascular and Endovascular Surgery: the Official Journal of the European Society for Vascular Surgery. 2004;27(5):456-465. - PubMed
-
- Abacı O, Kılıçkesmez KO. Aspirin resistance: where are we now? Anadolu Kardiyoloji Dergisi : AKD=the Anatolian Journal of Cardiology. 2013;13(4):370-373. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
