

Acquired pial arteriovenous fistula secondary to cerebral cortical vein thrombosis: A case report and review of the literature
- PMID: 34609931
- PMCID: PMC9437507
- DOI: 10.1177/19714009211049080
Acquired pial arteriovenous fistula secondary to cerebral cortical vein thrombosis: A case report and review of the literature
Abstract
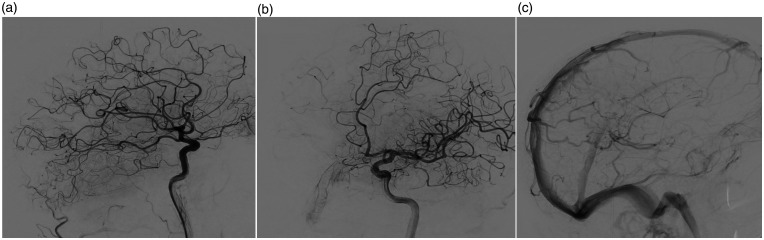
Pial arteriovenous fistulas (AVFs) are rare neurovascular malformations. They differ from arteriovenous malformations (AVMs) in that they involve single or multiple feeding arteries, draining directly into a dilated cortical vein with no intervening nidus. Pial and dural AVFs differ in blood supply, as the first originate from pial or cortical arteries and the latter from outside the dural leaflets. Unlike dural AVFs, most of the pial AVFs are supratentorial. The vast majority are congenital, manifesting during infancy. Acquired pial AVFs are significantly rarer and occur after vasculopathy, head trauma, brain surgery, or cerebral vein thrombosis. We describe a unique case of an acquired pial AVF in a 50-year-old man secondary to a cortical vein thrombosis manifesting as a focal-onset seizure with secondary generalization. A cerebral digital subtraction angiography revealed a low-flow pial AVF fed by a postcentral branch of the left middle cerebral artery draining to the superior sagittal sinus via a cortical vein. It also showed a collateral venous circulation adjacent to the previously thrombosed left parietal vein. There was no evidence of an associated dural AVF or venous varix. Endovascular treatment was scheduled three months later, but the angiogram preceding the embolization showed spontaneous and complete closure of the malformation. To our knowledge, this is the first case illustrating acquired pure pial AVF unaccompanied by a dural component following cortical vein thrombosis, eventually resulting in an unprompted closure.
Keywords: Pial arteriovenous fistula; cortical vein thrombosis; digital subtracted angiography; endovascular treatment.; magnetic resonance imaging.
Figures



Similar articles
-
Acquired pial and dural arteriovenous fistulae following superior sagittal sinus thrombosis in patients with protein S deficiency: a report of two cases.Neurol Med Chir (Tokyo). 2014;54(3):245-52. doi: 10.2176/nmc.cr2012-0311. Epub 2013 Oct 25. Neurol Med Chir (Tokyo). 2014. PMID: 24162240 Free PMC article. Review.
-
Multiple Cranial Dural and Pial Arteriovenous Fistulas with Occlusion of All After Embolization of Primary Superior Sagittal Sinus Dural Fistula.World Neurosurg. 2020 Aug;140:224-228. doi: 10.1016/j.wneu.2020.05.045. Epub 2020 May 11. World Neurosurg. 2020. PMID: 32437996
-
Dural and Pial Arteriovenous Fistulas Connected to the Same Drainer in the Middle Cranial Fossa: A Case Report.World Neurosurg. 2018 Oct;118:47-52. doi: 10.1016/j.wneu.2018.06.214. Epub 2018 Jul 5. World Neurosurg. 2018. PMID: 29981916
-
Acquired pial arteriovenous fistula following cerebral vein thrombosis.Stroke. 1999 Nov;30(11):2487-90. doi: 10.1161/01.str.30.11.2487. Stroke. 1999. PMID: 10548689
-
Multiple Dural and Pial Arteriovenous Fistulae in a Twenty-Four-Year-Old Woman in the Setting of Superior Sagittal Sinus Thrombosis: Case Report and Review of Literature.J Stroke Cerebrovasc Dis. 2016 Oct;25(10):e192-9. doi: 10.1016/j.jstrokecerebrovasdis.2016.07.037. Epub 2016 Aug 17. J Stroke Cerebrovasc Dis. 2016. PMID: 27544867 Review.
Cited by
-
Embolization of cerebellar pial arteriovenous fistula presented with congestive edema of the brainstem and cervical cord.Neuroradiol J. 2024 Dec;37(6):764-771. doi: 10.1177/19714009231224421. Epub 2023 Dec 22. Neuroradiol J. 2024. PMID: 38135276
-
Pial arteriovenous fistula with a large intraparenchymal hemorrhage in a 9-year-old child: a case report and case-based mini review.Childs Nerv Syst. 2025 Mar 17;41(1):132. doi: 10.1007/s00381-025-06784-7. Childs Nerv Syst. 2025. PMID: 40097751 Free PMC article. Review.
References
-
- Newton TH, Cronqvist S. Involvement of dural arteries in intracranial arteriovenous malformations. Radiology 1969; 93:1071–1078. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
