

The age-related decline in spatiotemporal gait characteristics is moderated by concerns of falling, history of falls & diseases, and sociodemographic-anthropometric characteristics in 60-94 years old adults
- PMID: 34610791
- PMCID: PMC8493753
- DOI: 10.1186/s11556-021-00275-9
The age-related decline in spatiotemporal gait characteristics is moderated by concerns of falling, history of falls & diseases, and sociodemographic-anthropometric characteristics in 60-94 years old adults
Abstract
Background: Associations between age, concerns or history of falling, and various gait parameters are evident. Limited research, however, exists on how such variables moderate the age-related decline in gait characteristics. The purpose of the present study was to investigate the moderating effects of concerns of falling (formerly referred to as fear of falling), history of falls & diseases, and sociodemographic characteristics on changes in gait characteristics with increasing age in the elderly.
Methods: In this individual participant level data re-analysis, data from 198 participants (n = 125 females) from 60 to 94 years of age were analysed (mean 73.9, standard deviation 7.7 years). Dependent variables were major spatiotemporal gait characteristics, assessed using a capacitive force measurement platform (zebris FDM-T). Age (independent variable) and the moderating variables concerns of falling (FES-I), gender/sex, history of falls and fall-related medical records, number of drugs daily taken, and body mass index were used in the statistical analysis. Hierarchical linear mixed moderation models (multilevel analysis) with stepwise (forward) modelling were performed.
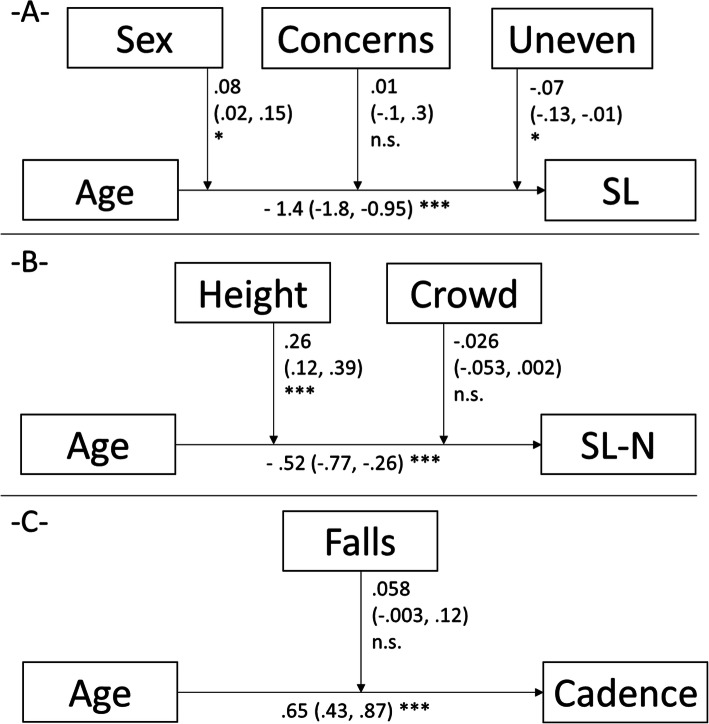
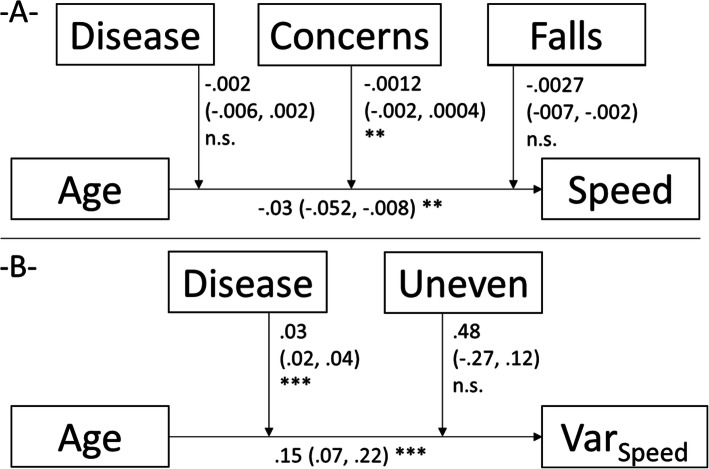
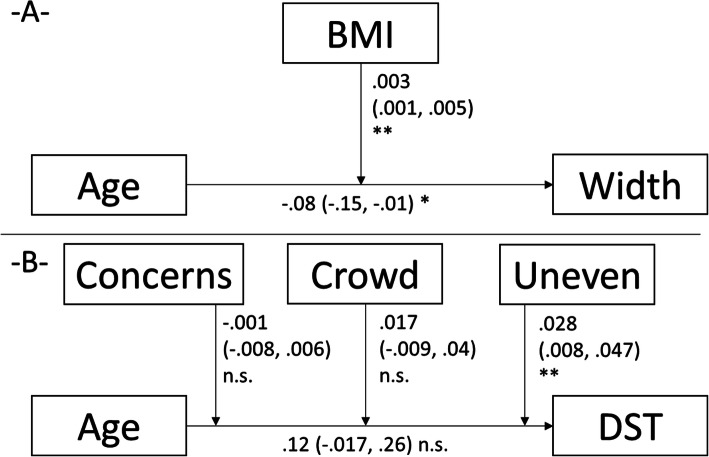
Results: Decreases of gait speed (estimate = -.03, equals a decrease of 0.03 m/s per year of ageing), absolute (- 1.4) and gait speed-normalized (-.52) stride length, step width (-.08), as well as increases in speed normalized cadence (.65) and gait speed variability (.15) are all age-related (each p < .05). Overall and specific situation-related concerns of falling (estimates: -.0012 to -.07) were significant moderators. History of potentially gait- and/or falls-affecting diseases accelerated the age-related decline in gait speed (-.002) and its variability (.03). History of falls was, although non-significant, a relevant moderator (in view of increasing the model fit) for cadence (.058) and gait speed (-.0027). Sociodemographics and anthropometrics showed further moderating effects (sex moderated the ageing effect on stride length, .08; height moderated the effect on the normalised stride length, .26; BMI moderated the effects on step width, .003). .
Conclusion: Age-related decline in spatiotemporal gait characteristics is moderated by concerns of falling, (non-significantly) by history of falls, significantly by history of diseases, and sociodemographic characteristics in 60-94 years old adults. Knowing the interactive contributions to gait impairments could be helpful for tailoring interventions for the prevention of falls.
Trial registration: Re-analysis of [21-24].
Keywords: Fall risk; Fear of falling; Older adults; Walking interaction.
© 2021. The Author(s).
Conflict of interest statement
None.
Figures
References
-
- Ageing and Life Course, Weltgesundheitsorganisation. WHO global report on falls prevention in older age. Geneva: World Health Organization Ageing and Life Course Family and Community Health; 2008.
LinkOut - more resources
Full Text Sources
Miscellaneous
