

Genomic and Transcriptomic Analysis of Relapsed and Refractory Childhood Solid Tumors Reveals a Diverse Molecular Landscape and Mechanisms of Immune Evasion
- PMID: 34610968
- PMCID: PMC10240575
- DOI: 10.1158/0008-5472.CAN-21-1033
Genomic and Transcriptomic Analysis of Relapsed and Refractory Childhood Solid Tumors Reveals a Diverse Molecular Landscape and Mechanisms of Immune Evasion
Abstract
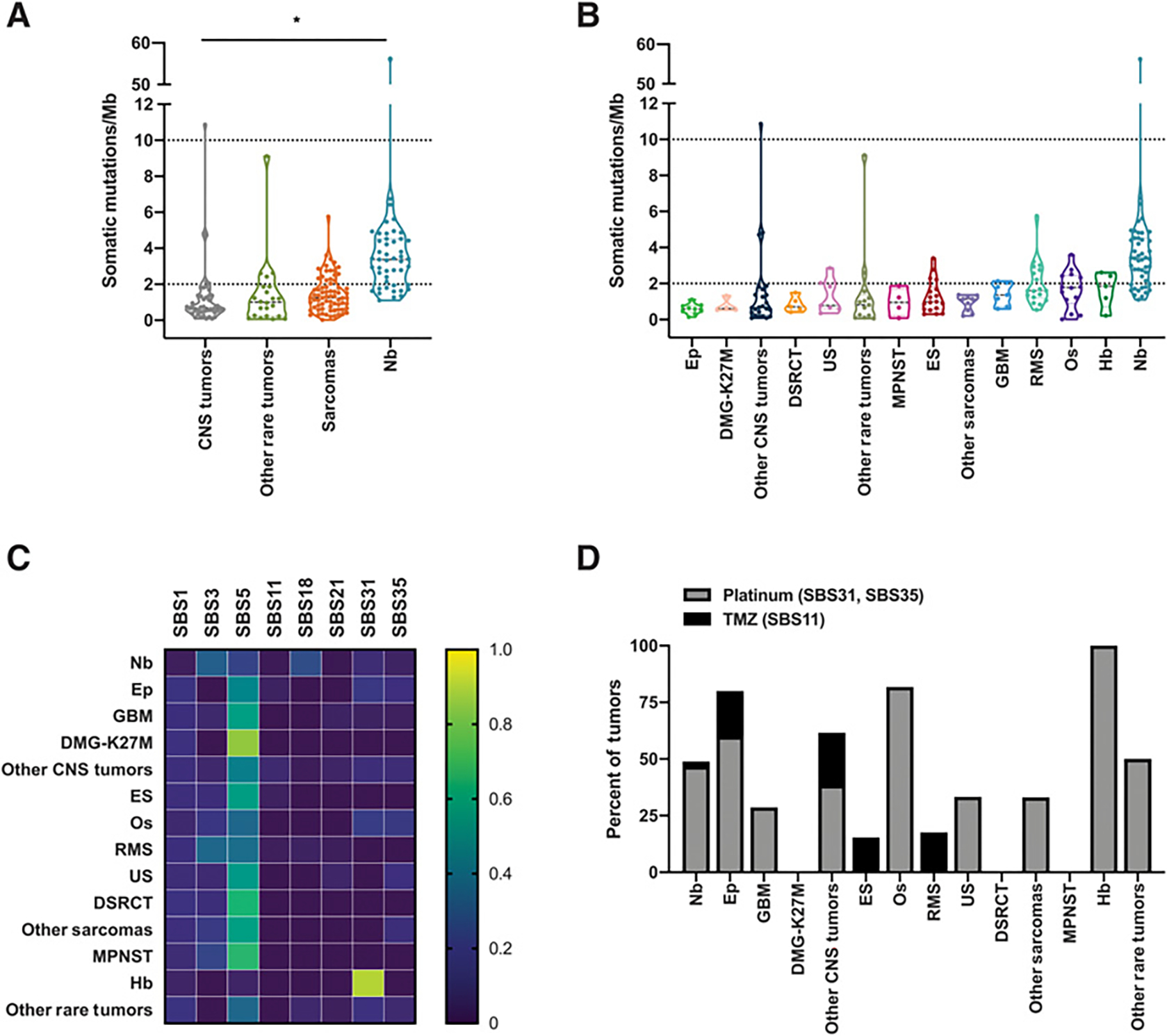
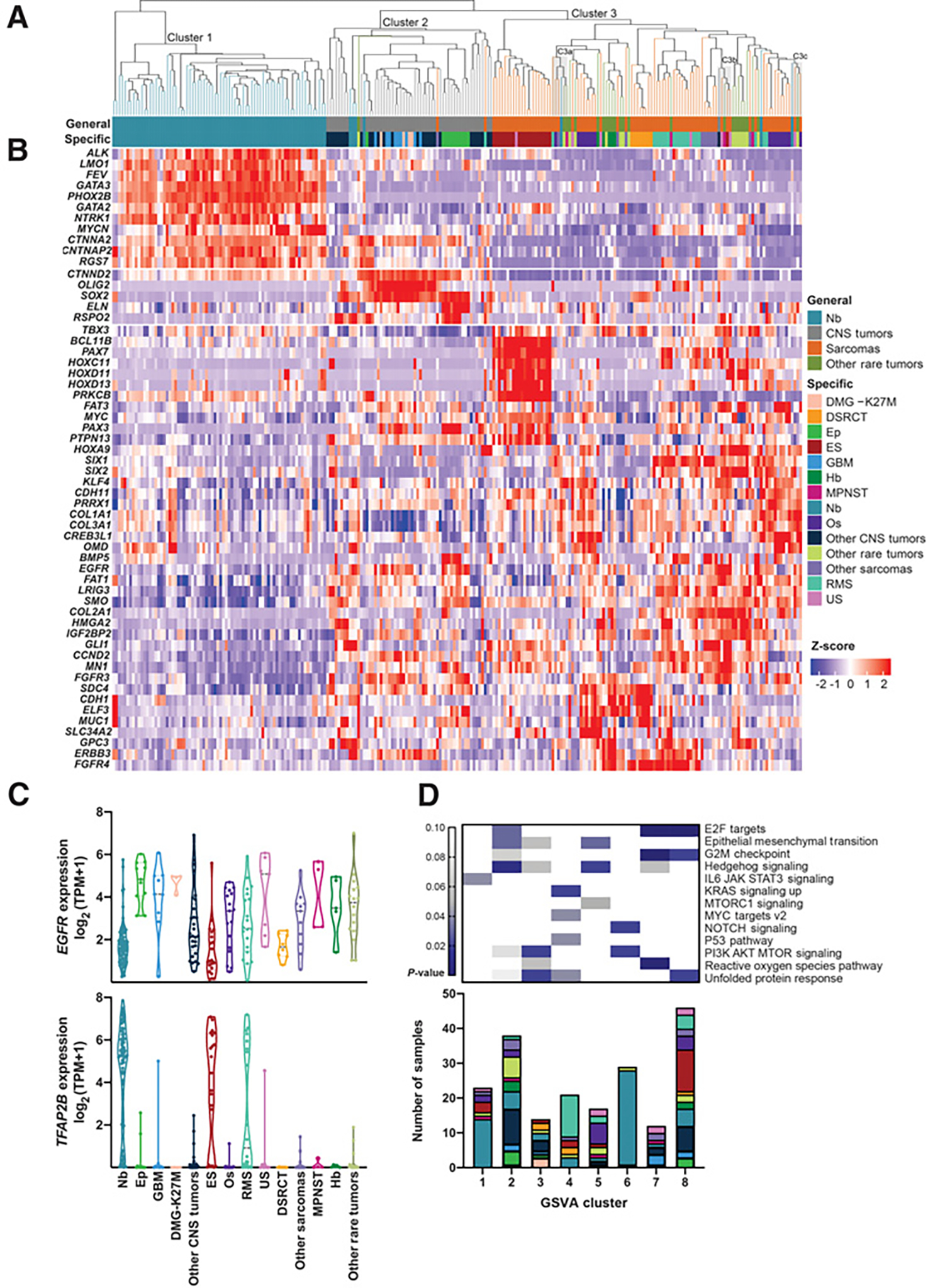
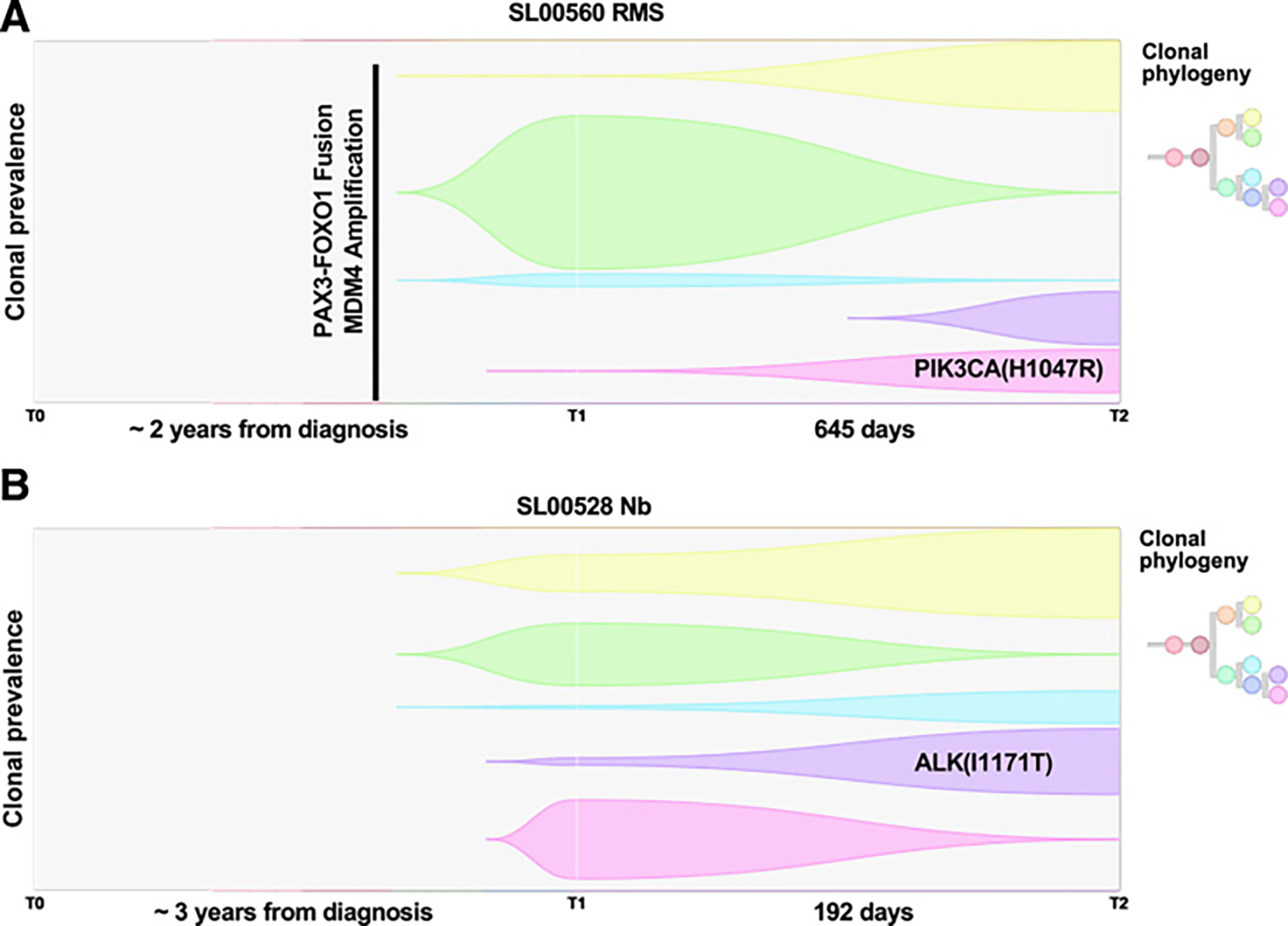
Children with treatment-refractory or relapsed (R/R) tumors face poor prognoses. As the genomic underpinnings driving R/R disease are not well defined, we describe here the genomic and transcriptomic landscapes of R/R solid tumors from 202 patients enrolled in Beat Childhood Cancer Consortium clinical trials. Tumor mutational burden (TMB) was elevated relative to untreated tumors at diagnosis, with one-third of tumors classified as having a pediatric high TMB. Prior chemotherapy exposure influenced the mutational landscape of these R/R tumors, with more than 40% of tumors demonstrating mutational signatures associated with platinum or temozolomide chemotherapy and two tumors showing treatment-associated hypermutation. Immunogenomic profiling found a heterogenous pattern of neoantigen and MHC class I expression and a general absence of immune infiltration. Transcriptional analysis and functional gene set enrichment analysis identified cross-pathology clusters associated with development, immune signaling, and cellular signaling pathways. While the landscapes of these R/R tumors reflected those of their corresponding untreated tumors at diagnosis, important exceptions were observed, suggestive of tumor evolution, treatment resistance mechanisms, and mutagenic etiologies of treatment. SIGNIFICANCE: Tumor heterogeneity, chemotherapy exposure, and tumor evolution contribute to the molecular profiles and increased mutational burden that occur in treatment-refractory and relapsed childhood solid tumors.
©2021 American Association for Cancer Research.
Figures


References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin 2020;70:7–30. - PubMed
-
- Grobner SN, Worst BC, Weischenfeldt J, Buchhalter I, Kleinheinz K, Rudneva VA, et al. The landscape of genomic alterations across childhood cancers. Nature 2018;555:321–7. - PubMed
-
- Wong M, Mayoh C, Lau LMS, Khuong-Quang DA, Pinese M, Kumar A, et al. Whole genome, transcriptome and methylome profiling enhances actionable target discovery in high-risk pediatric cancer. Nat Med 2020;26:1742–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
