

A simplified approach to identification of risk status in patients with atherosclerotic cardiovascular disease
- PMID: 34611633
- PMCID: PMC8387292
- DOI: 10.1016/j.ajpc.2021.100187
A simplified approach to identification of risk status in patients with atherosclerotic cardiovascular disease
Abstract
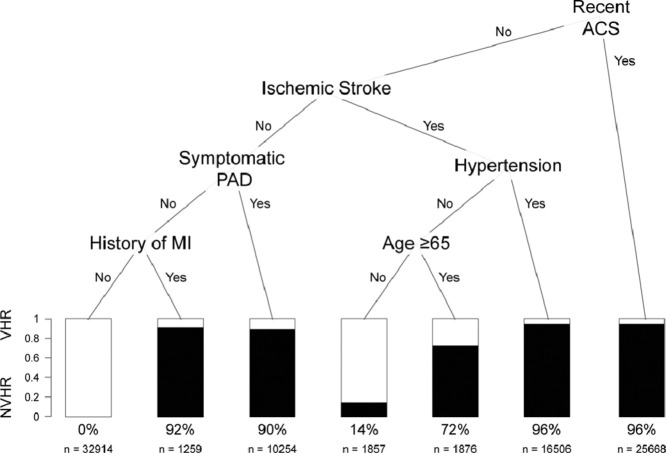
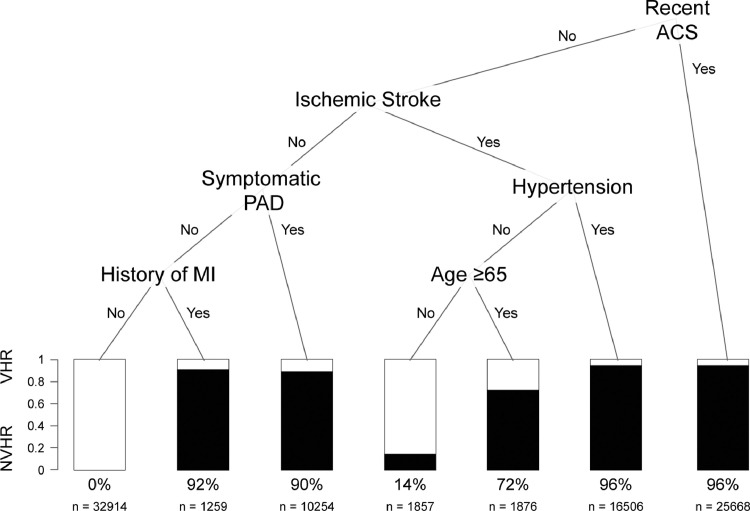
Objective: The 2018 American Heart Association/American College of Cardiology (AHA/ACC) Blood Cholesterol Guideline recommendation to classify patients with atherosclerotic cardiovascular disease (ASCVD) as very high-risk (VHR) vs not-VHR (NVHR) has important implications for escalation of medical therapy. We aimed to define the prevalence and clinical characteristics of these two groups within a large multi-state healthcare system and develop a simpler means to assist clinicians in identifying VHR patients using classification and regression tree (CART) analysis.
Methods: We performed a retrospective analysis of all patients in a 28-hospital US healthcare system in 2018. ICD-10 codes were used to define the ASCVD population. Per the AHA/ACC Guideline, VHR status was defined by ≥2 major ASCVD events or 1 major ASCVD event and ≥2 high-risk conditions. CART analysis was performed on training and validation datasets. A random forest model was used to verify results.
Results: Of 180,669 ASCVD patients identified, 58% were VHR. Among patients with a history of myocardial infarction (MI) or recent acute coronary syndrome (ACS), 99% and 96% were classified as VHR, respectively. Both CART and random forest models identified recent ACS, ischemic stroke, hypertension, peripheral artery disease, history of MI, and age as the most important predictors of VHR status. Using five rules identified by CART analysis, fewer than 50% of risk factors were required to assign VHR status.
Conclusion: CART analysis helped to streamline the identification of VHR patients based on a limited number of rules and risk factors. This approach may help improve clinical decision making by simplifying ASCVD risk assessment at the point of care. Further validation is needed, however, in more diverse populations.
Keywords: ASCVD; Cholesterol; Lipid; Secondary prevention.
© 2021 The Authors. Published by Elsevier B.V.
Conflict of interest statement
SSM: has current research support from the American Heart Association, PCORI, National Institutes of Health, the David and June Trone Family Foundation, and Pollin Digital Health Innovation Fund. He has served as a consultant to Astrazeneca, DalCor Pharmaceuticals, 89bio, Amgen, Esperion, Kaneka, and Sanofi. He has a patent System to estimate LDL cholesterol levels pending to Co-Inventor. He is a founder of and holds equity in Corrie Health, which intends to further develop the platform. SSV: Grant support: Department of Veterans Affairs, World Heart Federation, Tahir and Jooma Family; Honorarium: American College of Cardiology (Associate Editor for Innovations, acc.org); Steering Committee Member: Patient and Provider Assessment of Lipid Management (PALM) registry [no financial remuneration]. AS, HFL, KJS, AA, TJG: None.
Figures
References
-
- Grundy S.M., Stone N.J., Bailey A.L. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol. J Am Coll Cardiol. 2019;73(24):e285–e350. - PubMed
-
- Bayoumy K., Gaber M., Mani P. LDL-C targets in secondary prevention: how low should we go? Curr Cardiovasc Risk Rep. 2019;13(8):23.
-
- Sardar P., Abbott J.D., Kundu A., Aronow H.D., Granada J.F., Giri J. Impact of artificial intelligence on interventional cardiology. JACC Cardiovasc Interv. 2019;12(14):1293–1303. - PubMed
LinkOut - more resources
Full Text Sources
