

Tracking Blood Pressure Control Performance and Process Metrics in 25 US Health Systems: The PCORnet Blood Pressure Control Laboratory
- PMID: 34612048
- PMCID: PMC8751828
- DOI: 10.1161/JAHA.121.022224
Tracking Blood Pressure Control Performance and Process Metrics in 25 US Health Systems: The PCORnet Blood Pressure Control Laboratory
Abstract
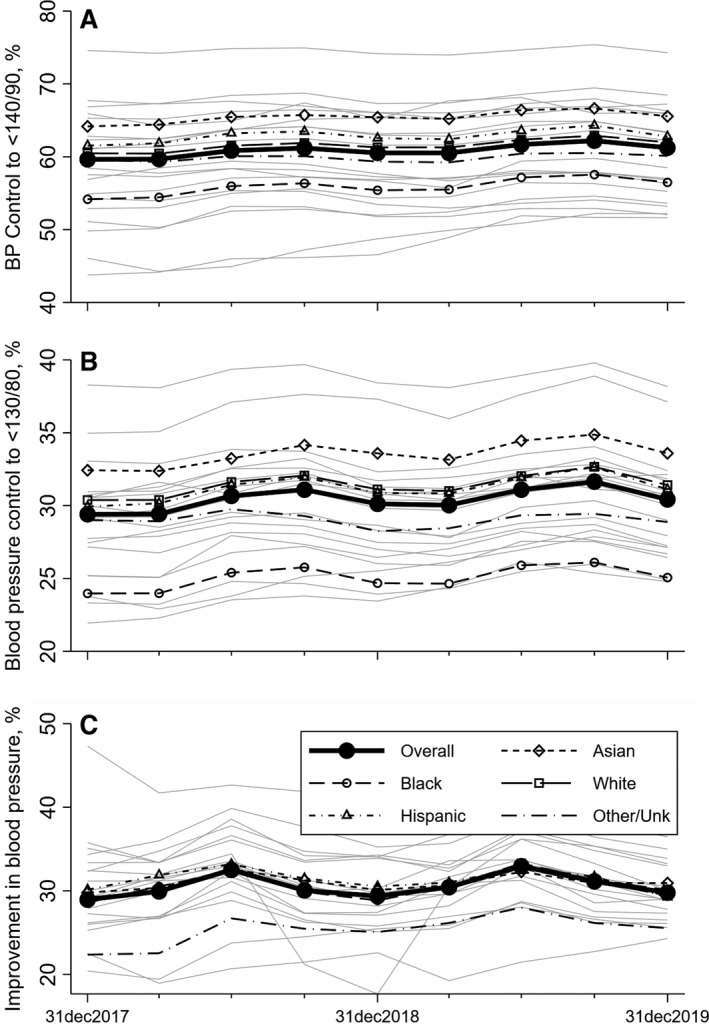
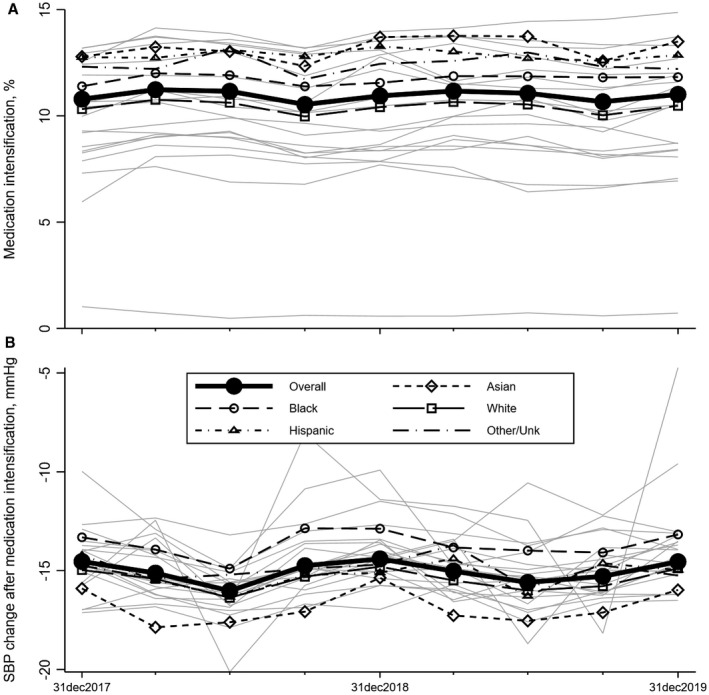
Background The National Patient-Centered Clinical Research Network Blood Pressure Control Laboratory Surveillance System was established to identify opportunities for blood pressure (BP) control improvement and to provide a mechanism for tracking improvement longitudinally. Methods and Results We conducted a serial cross-sectional study with queries against standardized electronic health record data in the National Patient-Centered Clinical Research Network (PCORnet) common data model returned by 25 participating US health systems. Queries produced BP control metrics for adults with well-documented hypertension and a recent encounter at the health system for a series of 1-year measurement periods for each quarter of available data from January 2017 to March 2020. Aggregate weighted results are presented overall and by race and ethnicity. The most recent measurement period includes data from 1 737 995 patients, and 11 956 509 patient-years were included in the trend analysis. Overall, 15% were Black, 52% women, and 28% had diabetes. BP control (<140/90 mm Hg) was observed in 62% (range, 44%-74%) but varied by race and ethnicity, with the lowest BP control among Black patients at 57% (odds ratio, 0.79; 95% CI, 0.66-0.94). A new class of antihypertensive medication (medication intensification) was prescribed in just 12% (range, 0.6%-25%) of patient visits where BP was uncontrolled. However, when medication intensification occurred, there was a large decrease in systolic BP (≈15 mm Hg; range, 5-18 mm Hg). Conclusions Major opportunities exist for improving BP control and reducing disparities, especially through consistent medication intensification when BP is uncontrolled. These data demonstrate substantial room for improvement and opportunities to close health equity gaps.
Keywords: health equity; high blood pressure; hypertension; quality and outcomes; race and ethnicity.
Figures
References
-
- Global Burden of Disease Risk Factors . Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1659–1724. doi: 10.1016/S0140-6736(16)31679-8 - DOI - PMC - PubMed
-
- Foraker RE, Benziger CP, DeBarmore BM, Cené CW, Loustalot F, Khan Y, Anderson CAM, Roger VL; Prevention AHACoEa, Council on Arteriosclerosis TraVB and Health aCoLaC . Achieving optimal population cardiovascular health requires an interdisciplinary team and a learning healthcare system: a scientific statement from the American Heart Association. Circulation. 2021;143:e9–e18. doi: 10.1161/CIR.0000000000000913 - DOI - PMC - PubMed
-
- Pletcher MJ, Fontil V, Carton T, Shaw KM, Smith M, Choi S, Todd J, Chamberlain AM, O’Brien EC, Faulkner M, et al. The PCORnet blood pressure control laboratory: a platform for surveillance and efficient trials. Circ Cardiovasc Qual Outcomes. 2020;13:e006115. doi: 10.1161/CIRCOUTCOMES.119.006115 - DOI - PMC - PubMed
