

A comparative analysis of deferoxamine treatment modalities for dermal radiation-induced fibrosis
- PMID: 34612609
- PMCID: PMC8572785
- DOI: 10.1111/jcmm.16913
A comparative analysis of deferoxamine treatment modalities for dermal radiation-induced fibrosis
Abstract
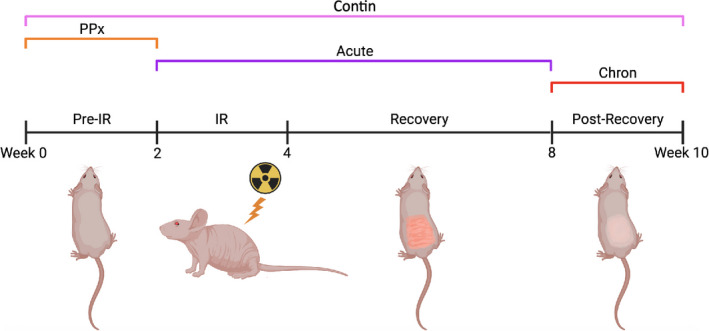
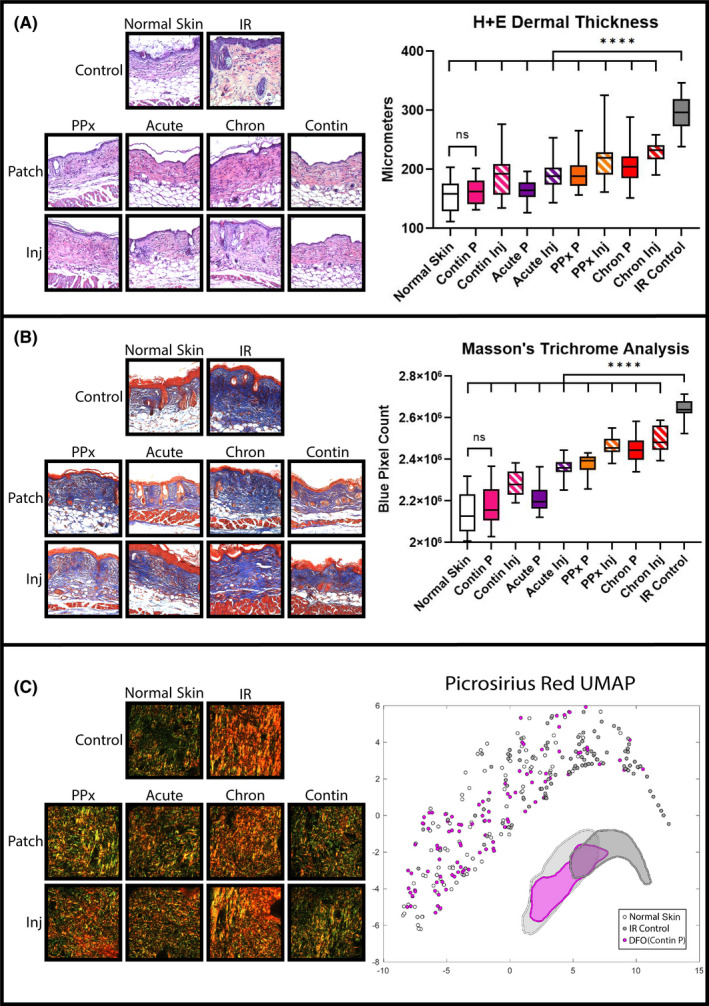
The iron chelator, deferoxamine (DFO), has been shown to potentially improve dermal radiation-induced fibrosis (RIF) in mice through increased angiogenesis and reduced oxidative damage. This preclinical study evaluated the efficacy of two DFO administration modalities, transdermal delivery and direct injection, as well as temporal treatment strategies in relation to radiation therapy to address collateral soft tissue fibrosis. The dorsum of CD-1 nude mice received 30 Gy radiation, and DFO (3 mg) was administered daily via patch or injection. Treatment regimens were prophylactic, during acute recovery, post-recovery, or continuously throughout the experiment (n = 5 per condition). Measures included ROS-detection, histology, biomechanics and vascularity changes. Compared with irradiated control skin, DFO treatment decreased oxidative damage, dermal thickness and collagen content, and increased skin elasticity and vascularity. Metrics of improvement in irradiated skin were most pronounced with continuous transdermal delivery of DFO. In summary, DFO administration reduces dermal fibrosis induced by radiation. Although both treatment modalities were efficacious, the transdermal delivery showed greater effect than injection for each temporal treatment strategy. Interestingly, the continuous patch group was more similar to normal skin than to irradiated control skin by most measures, highlighting a promising approach to address detrimental collateral soft tissue injury following radiation therapy.
Keywords: dermal fibrosis; fibrosis treatment; radiation therapy; translational science.
© 2021 The Authors. Journal of Cellular and Molecular Medicine published by Foundation for Cellular and Molecular Medicine and John Wiley & Sons Ltd.
Conflict of interest statement
Dr. Michael Longaker and Dr. Geoffrey Gurtner have equity stakes in TauTona Group, the DFO patch supplier. Dr. Geoffrey Gurtner holds a patent for topical and transdermal HIF‐1 modulators for chronic wound treatment. Dr. Derrick Wan, Dr. Michael Longaker and Dr. Geoffrey Gurtner hold a patent for the use of DFO in conditioning irradiated tissue.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
