

Transanal Drainage Tube Use for Preventing Anastomotic Leakage After Laparoscopic Low Anterior Resection in Patients With Rectal Cancer: A Randomized Clinical Trial
- PMID: 34613330
- PMCID: PMC8495603
- DOI: 10.1001/jamasurg.2021.4568
Transanal Drainage Tube Use for Preventing Anastomotic Leakage After Laparoscopic Low Anterior Resection in Patients With Rectal Cancer: A Randomized Clinical Trial
Abstract
Importance: Preventing anastomotic leakage (AL) is crucial for colorectal surgery. Some studies have suggested a positive role of transanal drainage tubes (TDTs) in AL prevention after low anterior resection, but this finding is controversial.
Objective: To assess the effect of TDTs in AL prevention after laparoscopic low anterior resection for rectal cancer.
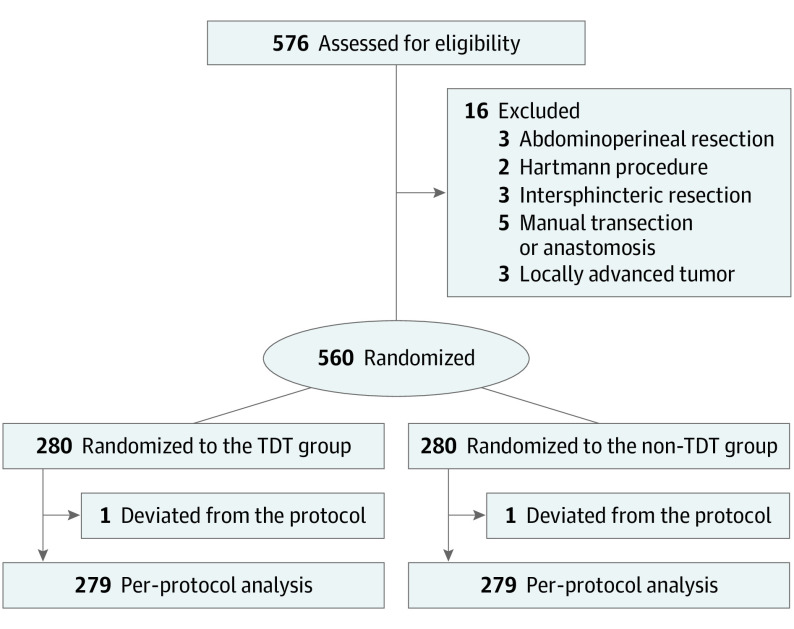
Design, setting, and participants: This multicenter randomized clinical trial with parallel groups (TDT vs non-TDT) was performed from February 26, 2016, to September 30, 2020. Participants included patients from 7 different hospitals in China who were undergoing laparoscopic low anterior resection with the double-stapling technique for mid-low rectal cancer; 576 patients were initially enrolled in this study, and 16 were later excluded. Ultimately, 560 patients were randomly divided between the TDT and non-TDT groups.
Interventions: A silicone tube was inserted through the anus, and the tip of the tube was placed approximately 5 cm above the anastomosis under laparoscopy at the conclusion of surgery. The tube was fixed with a skin suture and connected to a drainage bag. The TDT was scheduled for removal 3 to 7 days after surgery.
Main outcomes and measures: The primary end point was the postoperative AL rate within 30 days.
Results: In total, 576 patients were initially enrolled in this study; 16 of these patients were excluded. Ultimately, 560 patients were randomly divided between the TDT group (n = 280; median age, 61.5 years [IQR, 54.0-68.8 years]; 177 men [63.2%]) and the non-TDT group (n = 280; median age, 62.0 years [IQR, 52.0-69.0 years]; 169 men [60.4%]). Intention-to-treat analysis showed no significant difference between the TDT and non-TDT groups in AL rates (18 [6.4%] vs 19 [6.8%]; relative risk, 0.947; 95% CI, 0.508-1.766; P = .87) or AL grades (grade B, 14 [5.0%] and grade C, 4 [1.4%] vs grade B, 11 [3.9%] and grade C, 8 [2.9%]; P = .43). In the stratified analysis based on diverting stomas, there was no significant difference in the AL rate between the groups, regardless of whether a diverting stoma was present (without stoma, 12 [5.8%] vs 15 [7.9%], P = .41; and with stoma, 6 [8.3%] vs 4 [4.5%], P = .50). Anal pain was the most common complaint from patients in the TDT group (130 of 280, 46.4%). Accidental early TDT removal occurred in 20 patients (7.1%), and no bleeding or iatrogenic colonic perforations were detected.
Conclusions and relevance: The results from this randomized clinical trial indicated that TDTs may not confer any benefit for AL prevention in patients who undergo laparoscopic low anterior resection for mid-low rectal cancer without preoperative radiotherapy.
Trial registration: ClinicalTrials.gov Identifier: NCT02686567.
Conflict of interest statement
Figures
Comment in
-
Transanal Drainage Tubes-Prevention of Leaks or Unnecessary Sump?JAMA Surg. 2021 Dec 1;156(12):1158-1159. doi: 10.1001/jamasurg.2021.4569. JAMA Surg. 2021. PMID: 34613353 No abstract available.
-
Should Prophylactic Transanal Tube Drainage Be Continued in Colorectal Surgery?-Reply.JAMA Surg. 2022 Jun 1;157(6):547-548. doi: 10.1001/jamasurg.2021.7564. JAMA Surg. 2022. PMID: 35138337 No abstract available.
-
Should Prophylactic Transanal Tube Drainage Be Continued in Colorectal Surgery?JAMA Surg. 2022 Jun 1;157(6):546-547. doi: 10.1001/jamasurg.2021.7561. JAMA Surg. 2022. PMID: 35138339 No abstract available.
References
-
- Salvans S, Mayol X, Alonso S, et al. . Postoperative peritoneal infection enhances migration and invasion capacities of tumor cells in vitro: an insight into the association between anastomotic leak and recurrence after surgery for colorectal cancer. Ann Surg. 2014;260(5):939-943. doi:10.1097/SLA.0000000000000958 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
