

Complement catalyzing glomerular diseases
- PMID: 34613485
- PMCID: PMC8523427
- DOI: 10.1007/s00441-021-03485-w
Complement catalyzing glomerular diseases
Abstract
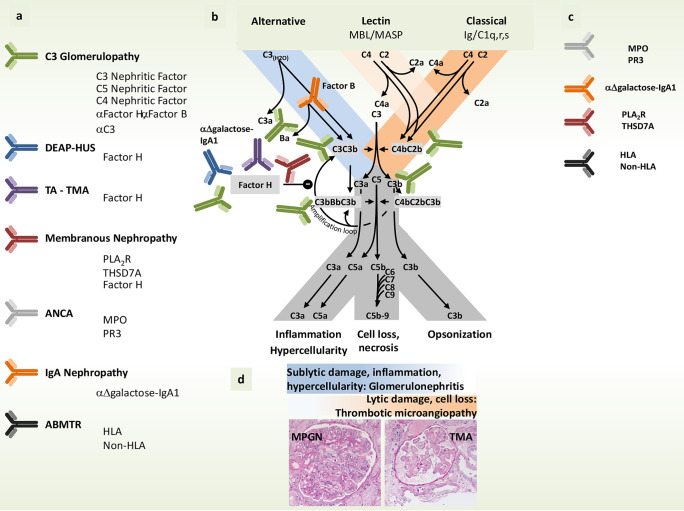
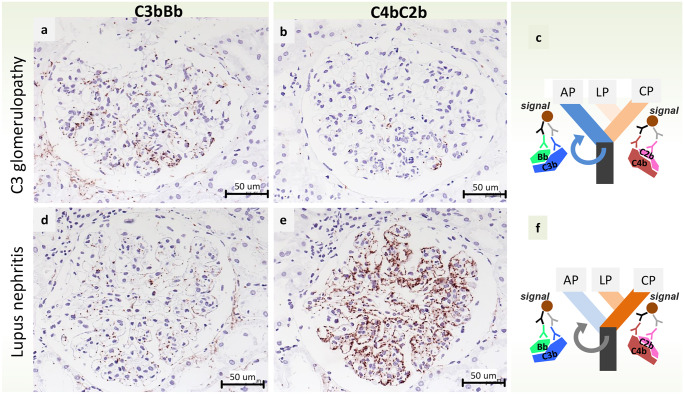
Complement is an evolutionarily conserved system which is important in the defense against microorganisms and also in the elimination of modified or necrotic elements of the body. Complement is activated in a cascade type manner and activation and all steps of cascade progression are tightly controlled and regulatory interleaved with many processes of inflammatory machinery. Overshooting of the complement system due to dysregulation can result in the two prototypes of primary complement mediated renal diseases: C3 glomerulopathy and thrombotic microangiopathy. Apart from these, complement also is highly activated in many other inflammatory native kidney diseases, such as membranous nephropathy, ANCA-associated necrotizing glomerulonephritis, and IgA nephropathy. Moreover, it likely plays an important role also in the transplant setting, such as in antibody-mediated rejection or in hematopoietic stem cell transplant associated thrombotic microangiopathy. In this review, these glomerular disorders are discussed with regard to the role of complement in their pathogenesis. The consequential, respective clinical trials for complement inhibitory therapy strategies for these diseases are described.
Keywords: C3 Convertase testing; C3 glomerulopathy; Complement; Complement diagnostics; Glomerular diseases; Thrombotic microangiopathy.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Bamoulid J, Roodenburg A, Staeck O, Wu K, Rudolph B, Brakemeier S, Halleck F, Lehner I, Schönemann C, Lachmann N, Budde K. Clinical outcome of patients with de novo C1q-binding donor-specific HLA antibodies after renal transplantation. Transplantation. 2017;101:2165–2174. doi: 10.1097/TP.0000000000001487. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
