

The Effects of Inhaled Airway Directed Pharmacotherapy on Decline in Lung Function Parameters Among Indigenous Australian Adults With and Without Underlying Airway Disease
- PMID: 34616149
- PMCID: PMC8487848
- DOI: 10.2147/COPD.S328137
The Effects of Inhaled Airway Directed Pharmacotherapy on Decline in Lung Function Parameters Among Indigenous Australian Adults With and Without Underlying Airway Disease
Abstract
Background: The trajectory of lung function decline among Indigenous patients with or without underlying chronic airway disease (COPD and concomitant bronchiectasis) and with use of inhaled pharmacotherapy, including inhaled corticosteroids (ICS), has not been reported in the past.
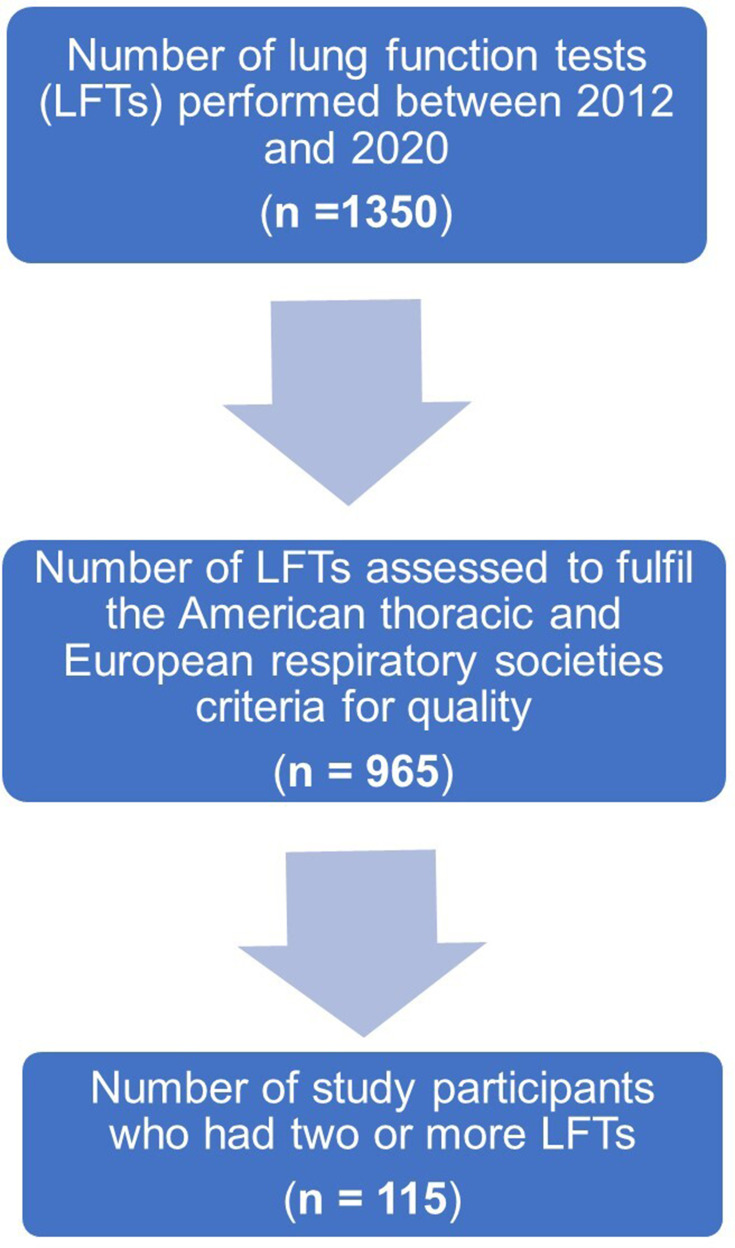
Methods: Adult Indigenous Australian patients identified to have undergone at least two or more lung function tests (LFTs) between 2012 and 2020 were assessed for changes in the lung function parameters (LFPs) between the first and last recorded LFTs.
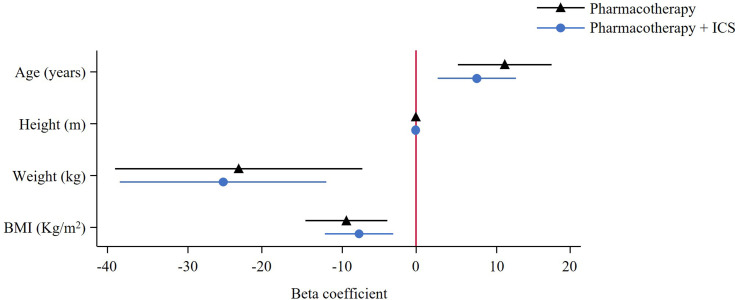
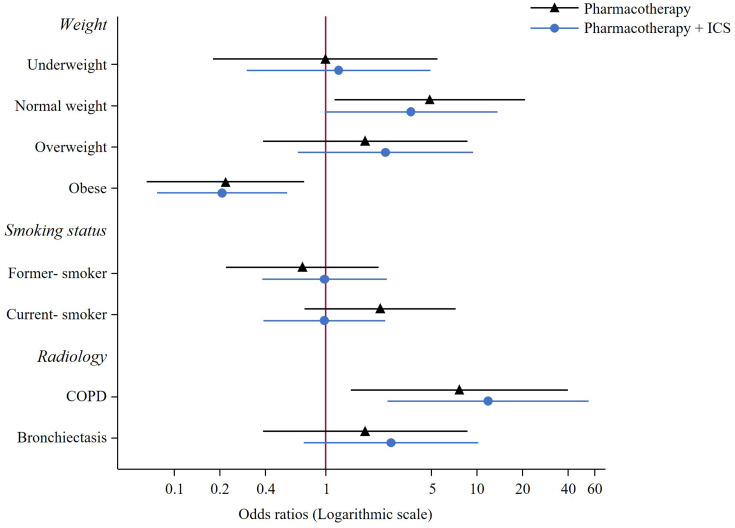
Results: Of the total 1350 patients identified to have undergone LFTs, 965 were assessed to fulfil session quality, 115 (n=58 females) were eligible to be included with two or more LFTs. Among the 115 patients, 49% showed radiological evidence of airway diseases, and 77% were on airway directed inhaled pharmacotherapy. Median time between LFTs was 1.5 years (IQR 0.86,5.85), with no significant differences in LFPs noted between first and last LFT. Overall rate of change (mL/year) showed considerable variation for FVC (median -37.55 mL/year [IQR -159.88,92.67]) and FEV1 (-18.74 mL/year [-102.49,71.44]) with minimal change in FEV1/FVC (0.00 ratio/year [-0.03,0.01]). When stratified by inhaled pharmacotherapy group, however, patients using ICS showed significantly greater rate of FEV1 decline (-48.64 mL/year [-110.18,62.5]) compared to those using pharmacotherapy with no ICS (15.46 mL/year [-73.5,74.62]) and those using no pharmacotherapy (-5.76 mL/year [-63.19,67.34]) (p=0.022). Additionally, a greater proportion of these patients reached the threshold for excessive FEV1 decline (64%) compared to those using pharmacotherapy without ICS (44%) and those using no pharmacotherapy (52%).
Conclusion: Decline in LFPs occurs commonly among adult Indigenous population, especially, excessive so among those using inhaled pharmacotherapy containing ICS.
Keywords: Aboriginal; COPD; ICS; LFT; bronchiectasis; indigenous; inhaled corticosteroids; lung function test.
© 2021 Heraganahally et al.
Conflict of interest statement
All authors declare no conflicts of interest for this study.
Figures
References
-
- Leading causes of mortality. Australian Institute of Health and Welfare 2020. Aboriginal and Torres Strait Islander Health Performance Framework 2020 summary report. Cat. no. IHPF 2. Canberra: AIHW. Available from:https://www.indigenoushpf.gov.au/publications/hpf-summary-2020. Accessed July5, 2021.
-
- Australian institute of health and welfare. Indigenous Australians more likely to die from CHD and COPD, but some positive trends emerging - Australian Institute of Health and Welfare; 2014. Available from:https://www.aihw.gov.au/news-media/media-releases/2014/june/indigenous-a.... Accessed July5, 2021.
-
- Australian institute of health and welfare. Asthma. Cat. no. ACM 33. Canberra: AIHW; 2020. Available from:https://www.aihw.gov.au/reports/chronic-respiratory-conditions/asthma. Accessed July5, 2021.
-
- Australian bureau of statistics. Estimates of Aboriginal and Torres Strait Islander Australians. Canberra, Australia: ABS; 2016.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
