

The Epidemiology of Lung Metastases
- PMID: 34616754
- PMCID: PMC8488106
- DOI: 10.3389/fmed.2021.723396
The Epidemiology of Lung Metastases
Abstract
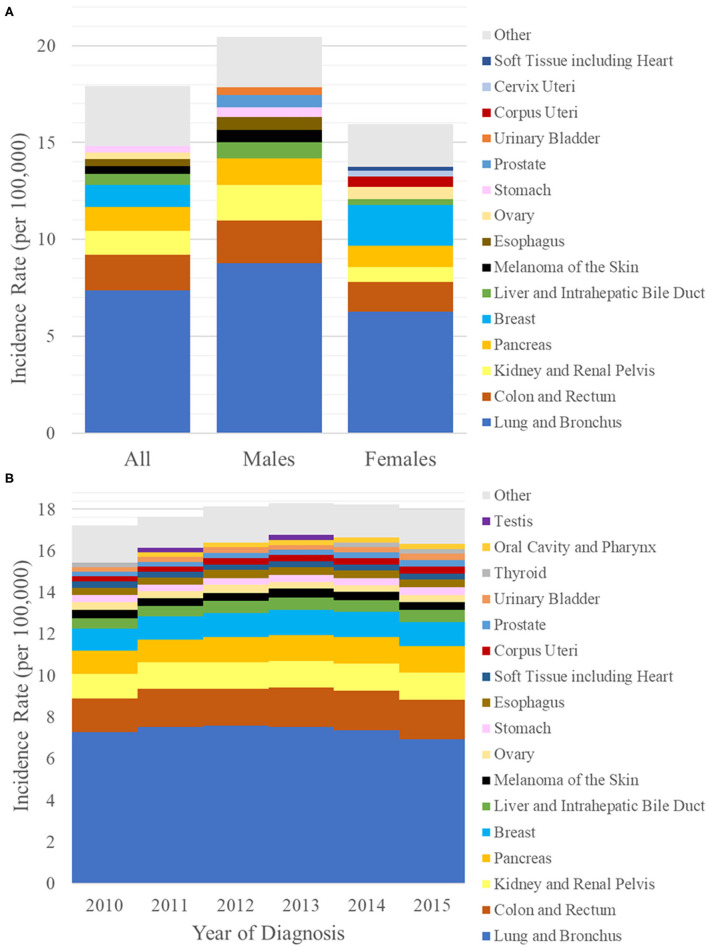
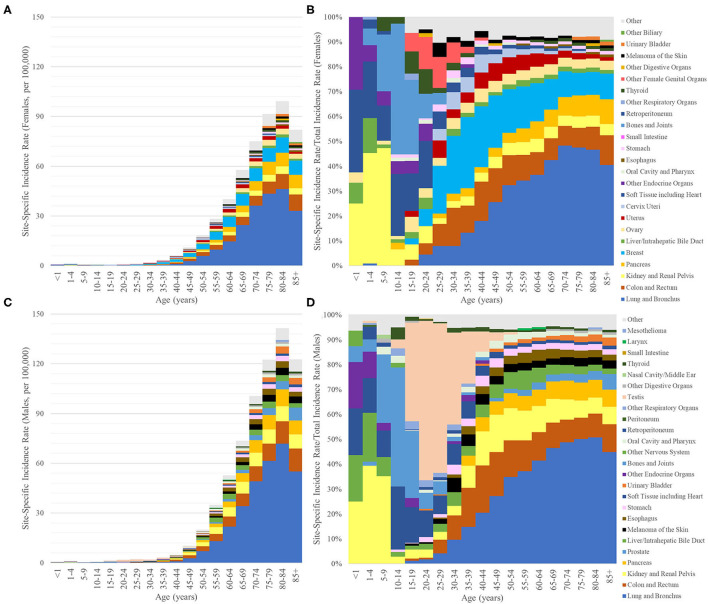
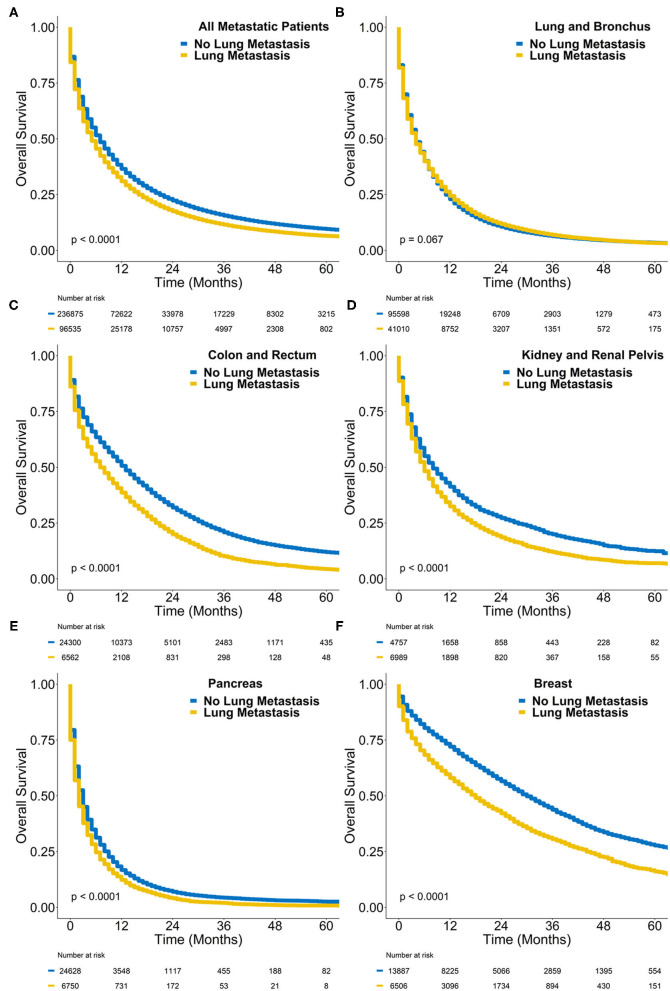
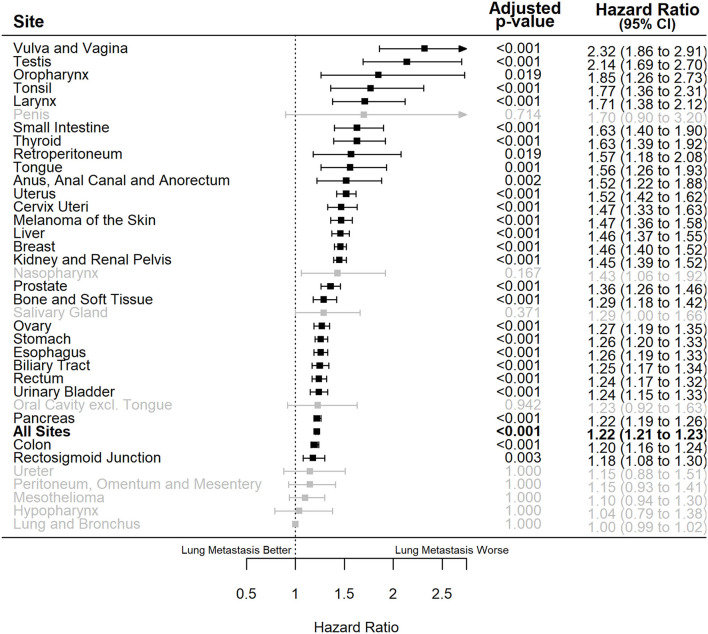
Introduction: Lung metastasis is usually associated with poor outcomes in cancer patients. This study was performed to characterize and analyze the population of patients with de novo (synchronous) lung metastases using the Surveillance, Epidemiology and End Results (SEER) database. Materials and Methods: Baseline characteristics of lung metastasis patients were obtained from SEER case listings. Incidence rates and counts of synchronous lung metastasis were also obtained using the SEER*Stat software. Survival outcomes were analyzed using univariate and multivariable Cox regressions, controlling for confounders. An alpha threshold of 0.05 was used for statistical significance and p-values were subject to correction for multiple comparisons. Results: The age-adjusted incidence rate of synchronous lung metastasis was 17.92 per 100,000 between 2010 and 2015. Synchronous lung metastases most commonly arose from primary lung cancers, colorectal cancers, kidney cancers, pancreatic cancers and breast cancers. During this time period, 4% of all cancer cases presented with synchronous lung metastasis. The percentage of patients presenting with synchronous lung metastasis ranged from 0.5% of all prostate cancers to 13% of all primary lung cancers. The percentage of all cancer cases presenting with synchronous lung metastasis increased over time. De novo metastatic patients with lung metastases had worse overall survival [hazard ratio = 1.22 (1.21-1.23), p < 0.001] compared to those with only extrapulmonary metastases, controlling for potential confounders. Conclusions: Synchronous lung metastasis occurs frequently and is an independent predictors of poor patient outcomes. As treatment for lung metastases becomes more complicated, patients with synchronous lung metastasis represent a high-risk population.
Keywords: cancer; epidemiology; lung cancer; metastases; oncology.
Copyright © 2021 Chen, Stoltzfus, Lehrer, Horn, Siva, Trifiletti, Meng, Verma, Louie and Zaorsky.
Conflict of interest statement
NZ received personal fees from Springer Nature Inc. and Weatherby Healthcare, unrelated to the submitted work. DT reports clinical trial research support from Novocure, and publishing fees from Springer Nature Inc. for projects unrelated to the submitted work. AL has received honoraria from Varian Medical Systems Inc. and AstraZeneca, unrelated to the current work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources