

Association between treatment-related lymphopenia and survival in glioblastoma patients following postoperative chemoradiotherapy
- PMID: 34617129
- PMCID: PMC9038819
- DOI: 10.1007/s00066-021-01855-5
Association between treatment-related lymphopenia and survival in glioblastoma patients following postoperative chemoradiotherapy
Abstract
Purpose: Our study investigated the association between treatment-related lymphopenia and overall survival (OS) in a series of glioblastoma (GBM) patients. We also explored clinical and dosimetric predictors of lymphocytes depletion.
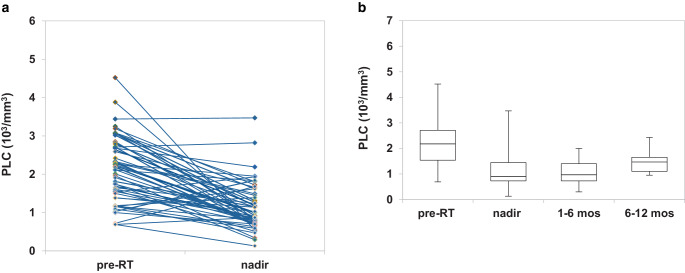
Methods: Between 2015 and 2019, 64 patients were treated at the same institution with postoperative chemoradiotherapy. Peripheral lymphocyte count (PLC) data and dose-volume histogram parameters were collected. Radiotherapy (RT) schedule consisted in standard total dose of 60 Gy in 30 daily fractions, with concomitant and adjuvant temozolomide (TMZ). Posttreatment acute absolute lymphopenia (nadir AAL) was calculated as a PLC lower than 1.0 × 103/mm3. Acute relative lymphopenia (ARL) was expressed by the nadir-PLC/baseline-PLC ratio < 0.5. Nadir-PLC was the lowest PLC registered between the end of RT and the first month of follow-up. Survival rates were estimated with Kaplan-Meier curves. Clinical and dosimetric variables related to AAL/ARL and OS were identified by univariate and multivariate analyses.
Results: A total of 57 patients were eligible and included in the analyses. The median PLC was significantly decreased following chemoradiotherapy (2180/mm3 vs 900/mm3). Median OS was 16 months (range 5-55 months), with no significant difference between patients who developed nadir AAL and those who did not (16 months vs 16.5 months; p = 0.304). When considering ARL vs non-ARL, median OS was 14 months vs 26 months (p = 0.013), respectively. In multivariate Cox regression only age, sex, extent of surgery, access to adjuvant chemotherapy and brain D98% were independently associated with OS.
Conclusion: Although iatrogenic immunosuppression could be associated with inferior clinical outcomes, our data show that treatment-related lymphopenia does not adversely affect GBM survival. Prospective studies are required to confirm these findings.
Keywords: Glioblastoma; Immunosuppression; Lymphopenia; Radiotherapy; Temozolomide.
© 2021. The Author(s).
Conflict of interest statement
R. Mapelli, C. Julita, S. P. Bianchi, N. Gallina, R. Lucchini, M. Midulla, F. Puci, J. Saddi, S. Trivellato, D. Panizza, E. De Ponti and S. Arcangeli declare that they have no competing interests.
Figures

References
-
- Shiraishi Y, Fang P, Xu C, Song J, Krishnan S, Koay EJ, Mehran RJ, Hofstetter WL, Blum-Murphy M, Ajani JA, Komaki R, Minsky B, Mohan R, Hsu CC, Hobbs BP, Lin SH. Severe lymphopenia during neoadjuvant chemoradiation for esophageal cancer: a propensity matched analysis of the relative risk of proton versus photon-based radiation therapy. Radiother Oncol. 2018;128(1):154–160. doi: 10.1016/j.radonc.2017.11.028. - DOI - PMC - PubMed
-
- Tang C, Liao Z, Gomez D, Levy L, Zhuang Y, Gebremichael RA, Hong DS, Komaki R, Welsh JW. Lymphopenia association with gross tumor volume and lung V5 and its effects on non-small cell lung cancer patient outcomes. Int J Radiat Oncol Biol Phys. 2014;89(5):1084–1091. doi: 10.1016/j.ijrobp.2014.04.025. - DOI - PubMed
-
- Wild AT, Ye X, Ellsworth SG, Smith JA, Narang AK, Garg T, Campian J, Laheru DA, Zheng L, Wolfgang CL, Tran PT, Grossman SA, Herman JM. The association between chemoradiation-related lymphopenia and clinical outcomes in patients with locally advanced pancreatic adenocarcinoma. Am J Clin Oncol. 2015;38(3):259–265. doi: 10.1097/COC.0b013e3182940ff9. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
