

Development and Evaluation of a Virtual Population of Children with Obesity for Physiologically Based Pharmacokinetic Modeling
- PMID: 34617262
- PMCID: PMC8813791
- DOI: 10.1007/s40262-021-01072-4
Development and Evaluation of a Virtual Population of Children with Obesity for Physiologically Based Pharmacokinetic Modeling
Abstract
Background and objective: While one in five children in the USA are now obese, and more than three-quarters receive at least one drug during childhood, there is limited dosing guidance for this vulnerable patient population. Physiologically based pharmacokinetic modeling can bridge the gap in the understanding of how pharmacokinetics, including drug distribution and clearance, changes with obesity by incorporating known obesity-related physiological changes in children. The objective of this study was to develop a virtual population of children with obesity to enable physiologically based pharmacokinetic modeling, then use the novel virtual population in conjunction with previously developed models of clindamycin and trimethoprim/sulfamethoxazole to better understand dosing of these drugs in children with obesity.
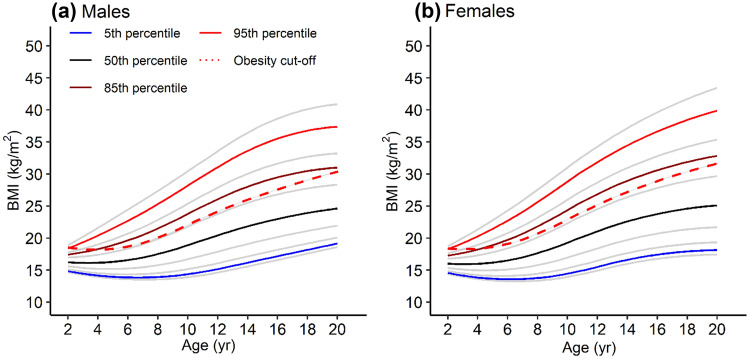
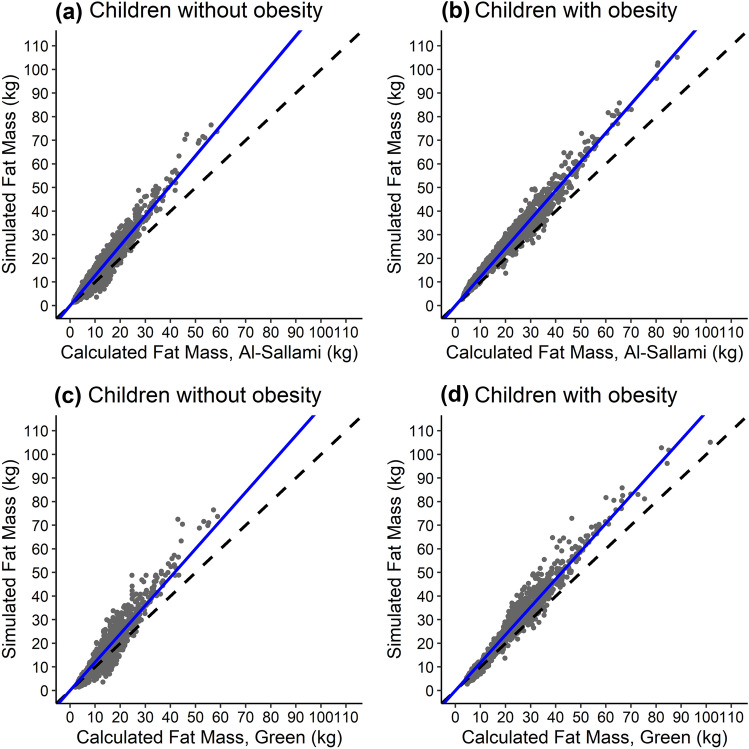
Methods: To enable physiologically based pharmacokinetic modeling, a virtual population of children with obesity was developed using national survey, electronic health record, and clinical trial data, as well as data extracted from the literature. The virtual population accounts for key obesity-related changes in physiology relevant to pharmacokinetics, including increased body size, body composition, organ size and blood flow, plasma protein concentrations, and glomerular filtration rate. The virtual population was then used to predict the pharmacokinetics of clindamycin and trimethoprim/sulfamethoxazole in children with obesity using previously developed physiologically based pharmacokinetic models.
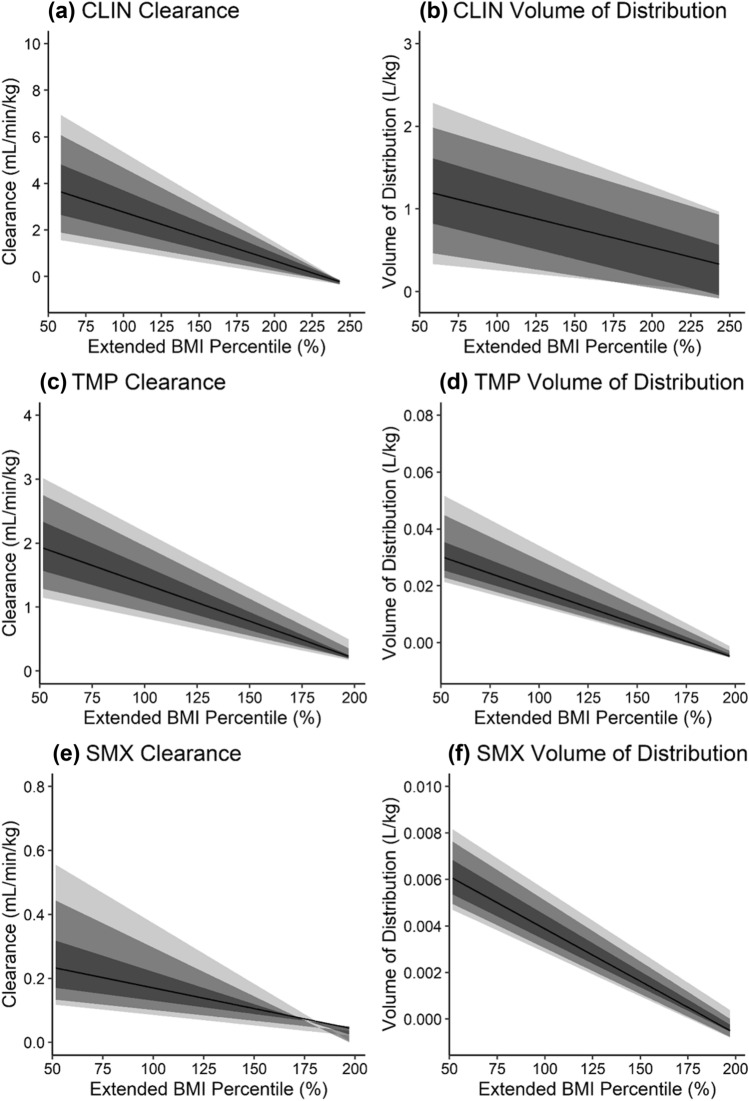
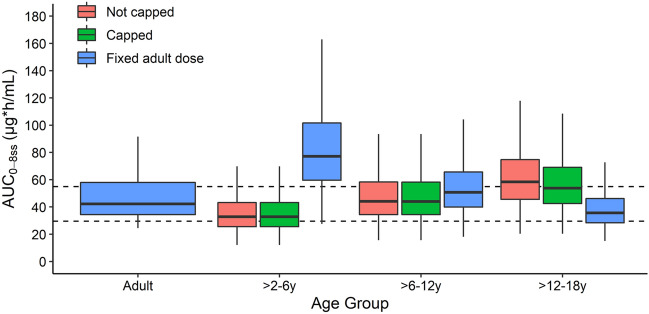
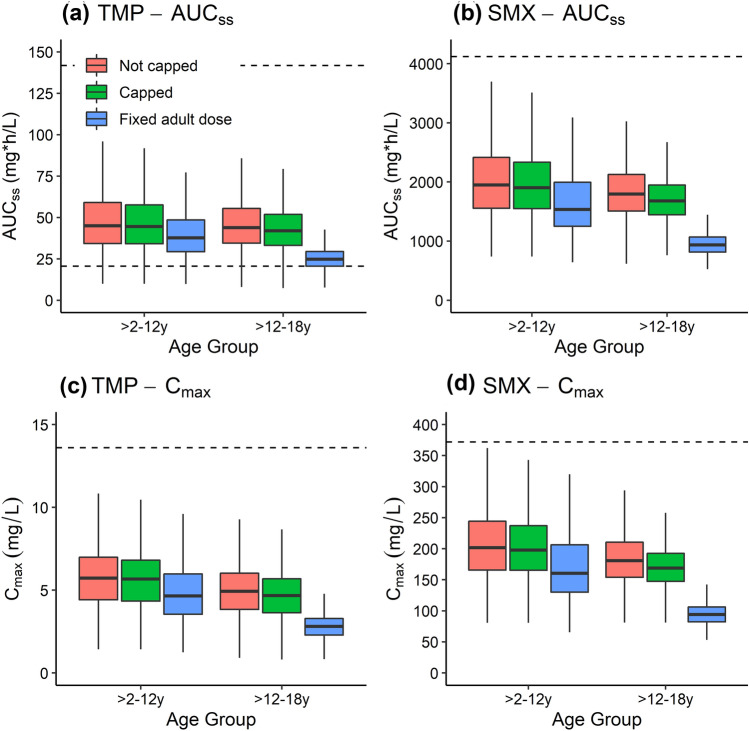
Results: Model simulations predicted observed concentrations well, with an overall average fold error of 1.09, 1.24, and 1.53 for clindamycin, trimethoprim, and sulfamethoxazole, respectively. Relative to children without obesity, children with obesity experienced decreased clindamycin and trimethoprim/sulfamethoxazole weight-normalized clearance and volume of distribution, and higher absolute doses under recommended pediatric weight-based dosing regimens.
Conclusions: Model simulations support current recommended weight-based dosing in children with obesity for clindamycin and trimethoprim/sulfamethoxazole, as they met target exposure despite these changes in clearance and volume of distribution.
© 2021. The Author(s).
Conflict of interest statement
M.C.-W. received support from the NICHD (HHSN275201000003I), the National Center for Advancing Translational Sciences [1U24TR001608]), and the FDA (1U18FD006298); he also receives research support from industry for neonatal and pediatric drug development,
Figures
References
-
- World Health Organization. Report of the commision on ending childhood obesity. WHO Doc Prod Serv. 2016. https://apps.who.int/iris/bitstream/handle/10665/204176/9789241510066_en.... Accessed 14 Nov 2020.
-
- Vernacchio L, Kelly JP, Kaufman DW, Mitchell AA. Medication use among children < 12 years of age in the United States: results from the Slone Survey. Pediatrics. 2009;124:446–454. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
