

Interleukin-1 blockade with anakinra and heart failure following ST-segment elevation myocardial infarction: results from a pooled analysis of the VCUART clinical trials
- PMID: 34617567
- PMCID: PMC9366639
- DOI: 10.1093/ehjcvp/pvab075
Interleukin-1 blockade with anakinra and heart failure following ST-segment elevation myocardial infarction: results from a pooled analysis of the VCUART clinical trials
Abstract
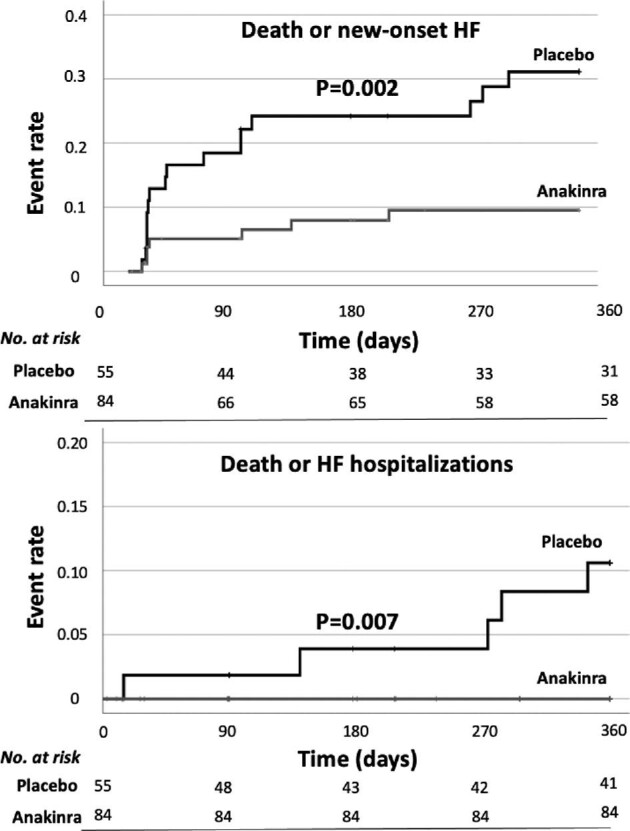
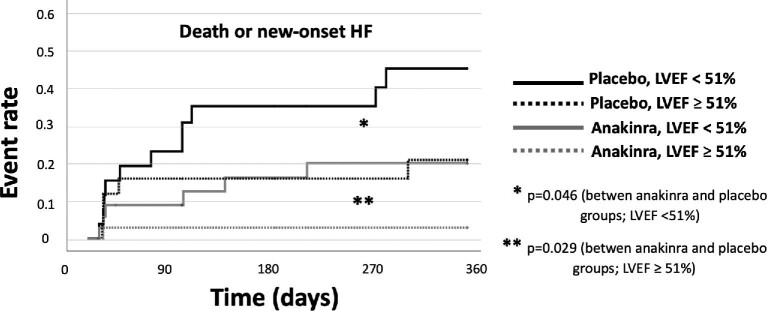
Aims: ST-segment elevation myocardial infarction (STEMI) is associated with an intense acute inflammatory response and an increased risk of death and heart failure (HF). In this study, we sought to evaluate the effect of anakinra, a recombinant interleukin-1 receptor antagonist, on the incidence of HF.
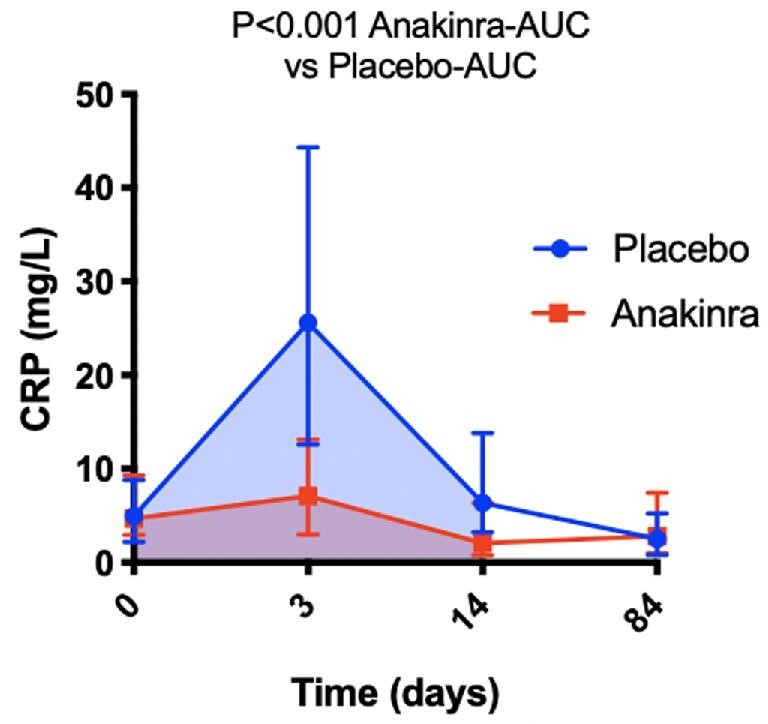
Methods and results: We performed a pooled analysis of three early phase randomized clinical trials. The endpoints included the composite of all-cause death and new-onset HF, and the composite of all-cause death and hospitalization for HF at 1-year follow-up. Safety events, including injection site reaction and serious infections, were also recorded. We analysed 139 patients with STEMI from three separate trials: VCUART (N = 10), VCUART2 (N = 30), and VCUART3 (N = 99). Of these, 84 (60%) patients were randomized to anakinra and 55 (40%) to placebo. Treatment with anakinra significantly reduced the incidence of all-cause death or new-onset HF (7 [8.2%] vs. 16 [29.1%], log-rank P = 0.002) and of all-cause death or HF hospitalization (0 [0] vs. 5 [9.1%], log-rank P = 0.007). Patients treated with anakinra had significantly higher injection site reactions (19 [22.6%] vs. 3 [5.5%], P = 0.016) without a significant difference in the incidence of serious infections (11 [13.1%] vs. 7 [12.7%], P = 0.435). Treatment with anakinra significantly reduced the area under the curve for high-sensitivity C-reactive protein between baseline and 14 days (75.48 [41.7-147.47] vs. 222.82 [117.22-399.28] mg day/L, P < 0.001).
Conclusion: IL-1 blockade with anakinra for 14 days in patients with STEMI reduces the incidence of new-onset HF or hospitalization for HF at 1 year following STEMI.
Keywords: Anakinra; Heart failure; Inflammation; Interleukin-1; STEMI.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Cung TT, Morel O, Cayla G, Rioufol G, Garcia-Dorado D, Angoulvant D, Bonnefoy-Cudraz E, Guérin P, Elbaz M, Delarche N, Coste P, Vanzetto G, Metge M, Aupetit JF, Jouve B, Motreff P, Tron C, Labeque JN, Steg PG, Cottin Y, Range G, Clerc J, Claeys MJ, Coussement P, Prunier F, Moulin F, Roth O, Belle L, Dubois P, Barragan P, Gilard M, Piot C, Colin P, De Poli F, Morice MC, Ider O, Dubois-Randé JL, Unterseeh T, Le Breton H, Béard T, Blanchard D, Grollier G, Malquarti V, Staat P, Sudre A, Elmer E, Hansson MJ, Bergerot C, Boussaha I, Jossan C, Derumeaux G, Mewton N, Ovize M. Cyclosporine before PCI in patients with acute myocardial infarction. N Engl J Med 2015;373:1021–1031. - PubMed
-
- Ezekowitz JA, Kaul P, Bakal JA, Armstrong PW, Welsh RC, McAlister FA. Declining in-hospital mortality and increasing heart failure incidence in elderly patients with first myocardial infarction. J Am Coll Cardiol 2009;53:13–20. - PubMed
-
- Mathur A, Fernández-Avilés F, Bartunek J, Belmans A, Crea F, Dowlut S, Galiñanes M, Good MC, Hartikainen J, Hauskeller C, Janssens S, Kala P, Kastrup J, Martin J, Menasché P, Sanz-Ruiz R, Ylä-Herttuala S, Zeiher A; BAMI Group . The effect of intracoronary infusion of bone marrow-derived mononuclear cells on all-cause mortality in acute myocardial infarction: the BAMI trial. Eur Heart J 2020;41:3702–3710. - PMC - PubMed
-
- Mewton N, Roubille F, Bresson D, Prieur C, Bouleti C, Bochaton T, Ivanes F, Dubreuil O, Biere L, Hayek A, Derimay F, Akodad M, Alos B, Haider L, El Jonhy N, Daw R, De Bourguignon C, Dhelens C, Finet G, Bonnefoy-Cudraz E, Bidaux G, Boutitie F, Maucort-Boulch D, Croisille P, Rioufol G, Prunier F, Angoulvant D. Effect of colchicine on myocardial injury in acute myocardial infarction. Circulation 2021;144:859–869. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
