

COVID-19 transmission dynamics underlying epidemic waves in Kenya
- PMID: 34618602
- PMCID: PMC7612211
- DOI: 10.1126/science.abk0414
COVID-19 transmission dynamics underlying epidemic waves in Kenya
Abstract
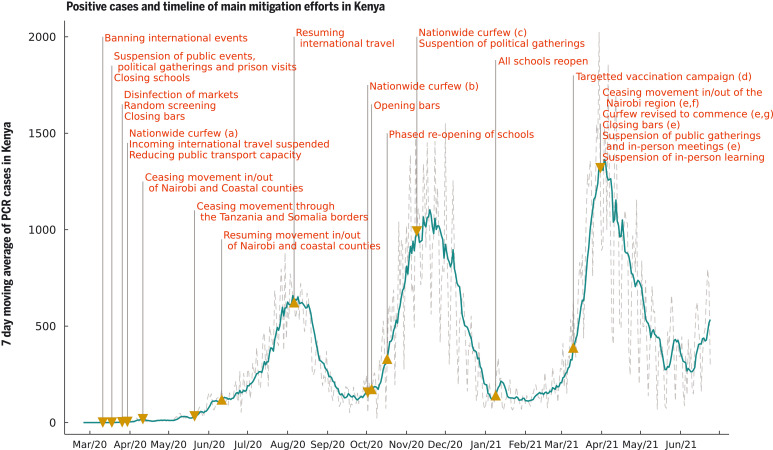
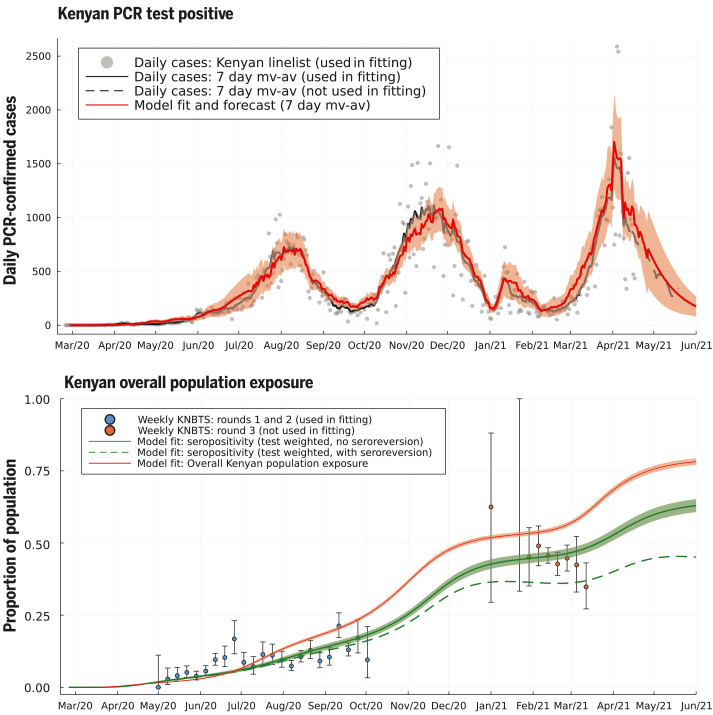
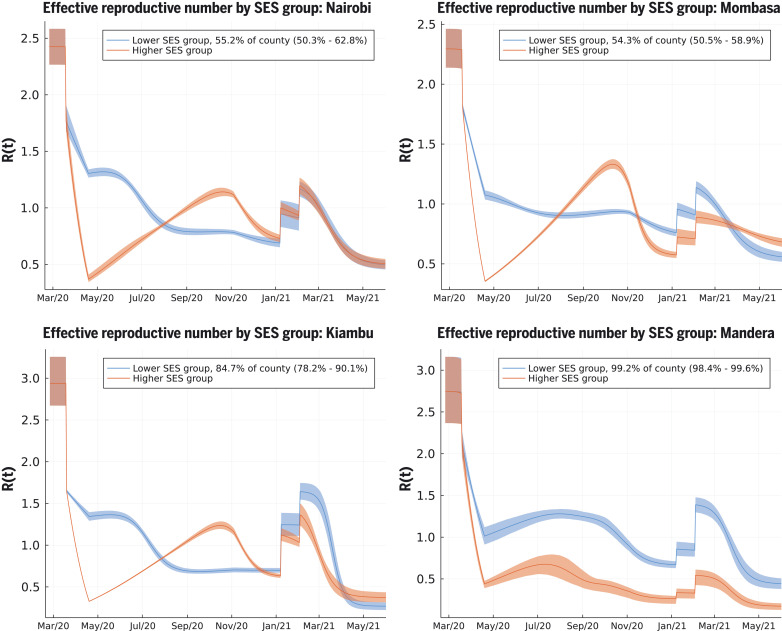
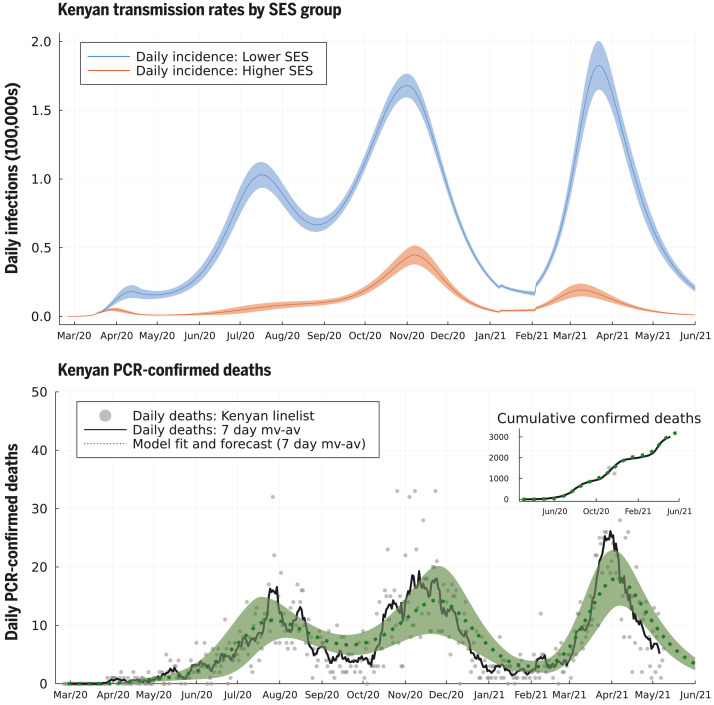
Policy decisions on COVID-19 interventions should be informed by a local, regional and national understanding of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission. Epidemic waves may result when restrictions are lifted or poorly adhered to, variants with new phenotypic properties successfully invade, or infection spreads to susceptible subpopulations. Three COVID-19 epidemic waves have been observed in Kenya. Using a mechanistic mathematical model, we explain the first two distinct waves by differences in contact rates in high and low social-economic groups, and the third wave by the introduction of higher-transmissibility variants. Reopening schools led to a minor increase in transmission between the second and third waves. Socioeconomic and urban–rural population structure are critical determinants of viral transmission in Kenya.
Figures
References
-
- E. Barasa et al., “Assessing the Indirect Health Effects of the COVID-19 Pandemic in Kenya” (2021); https://www.cgdev.org/publication/assessing-indirect-health-effects-covi.... - PMC - PubMed
-
- Uyoga S., Adetifa I. M. O., Karanja H. K., Nyagwange J., Tuju J., Wanjiku P., Aman R., Mwangangi M., Amoth P., Kasera K., Ng’ang’a W., Rombo C., Yegon C., Kithi K., Odhiambo E., Rotich T., Orgut I., Kihara S., Otiende M., Bottomley C., Mupe Z. N., Kagucia E. W., Gallagher K. E., Etyang A., Voller S., Gitonga J. N., Mugo D., Agoti C. N., Otieno E., Ndwiga L., Lambe T., Wright D., Barasa E., Tsofa B., Bejon P., Ochola-Oyier L. I., Agweyu A., Scott J. A. G., Warimwe G. M., Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Kenyan blood donors. Science 371, 79–82 (2021). 10.1126/science.abe1916 - DOI - PMC - PubMed
-
- S. P. C. Brand et al., Forecasting the scale of the COVID-19 epidemic in Kenya. medRxiv 2020.04.09.20059865 [Preprint]. 16 April 2020. 10.1101/2020.04.09.20059865 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
