

COVID-19 and metabolic disease: mechanisms and clinical management
- PMID: 34619105
- PMCID: PMC8489878
- DOI: 10.1016/S2213-8587(21)00244-8
COVID-19 and metabolic disease: mechanisms and clinical management
Abstract
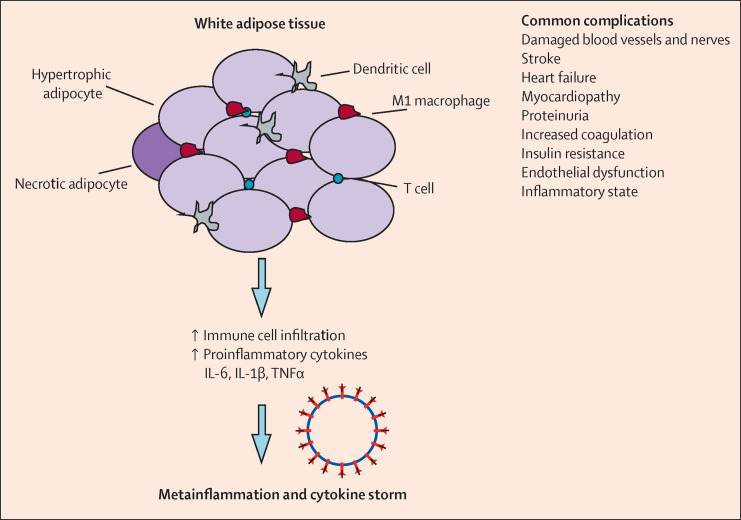
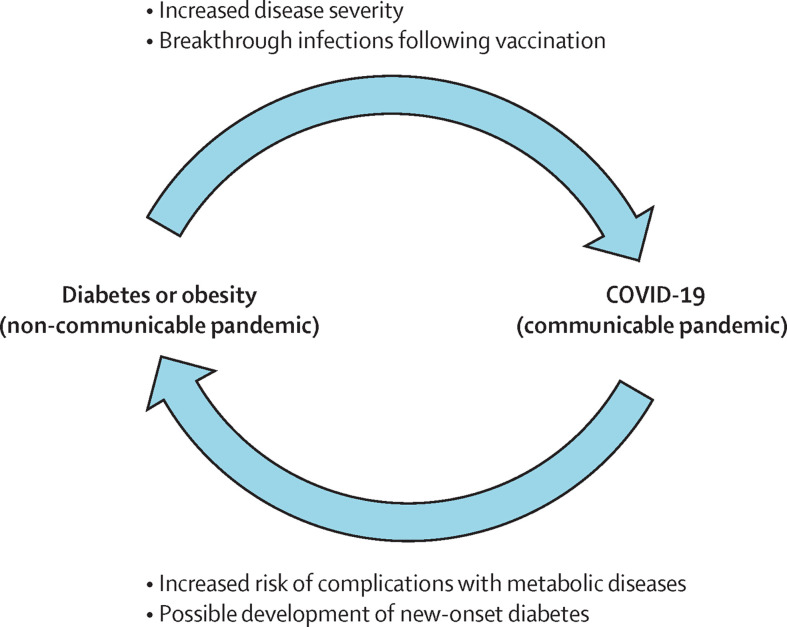
Up to 50% of the people who have died from COVID-19 had metabolic and vascular disorders. Notably, there are many direct links between COVID-19 and the metabolic and endocrine systems. Thus, not only are patients with metabolic dysfunction (eg, obesity, hypertension, non-alcoholic fatty liver disease, and diabetes) at an increased risk of developing severe COVID-19 but also infection with SARS-CoV-2 might lead to new-onset diabetes or aggravation of pre-existing metabolic disorders. In this Review, we provide an update on the mechanisms of how metabolic and endocrine disorders might predispose patients to develop severe COVID-19. Additionally, we update the practical recommendations and management of patients with COVID-19 and post-pandemic. Furthermore, we summarise new treatment options for patients with both COVID-19 and diabetes, and highlight current challenges in clinical management.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests KK reports acting as a consultant or speaker, or receiving grants for investigator-initiated studies for AstraZeneca, Novartis, Novo Nordisk, Sanofi-Aventis, Lilly and Merck Sharp & Dohme, Boehringer Ingelheim, Bayer, Berlin-Chemie AG–Menarini Group, Janssen, and Napp. JSS reports personal fees as a consultant or advisor for Abvance, Adocia, Astra-Zeneca, Avotres, Bayer, Biozeus, Boehringer-Ingelheim, Dalcor, Dance Biopharm–Aerami Therapeutics, Diavacs, Duologics, Elcelyx, Eli Lilly, Enthera, Esperion, Geneuro, Ideal Life, Imcyse, Immunomolecular Therapeutics, Intarcia, Kamada, Kriya, Moerae Matrix, Novo-Nordisk, Oramed, Orgenesis, Pila Pharma, Precigen ActoBiotics, Preziba/Signos, Provention Bio, Sanofi, Tolerion, Valeritas, Viacyte, Viela Bio, vTv Therapeutics, and Zafgen. JHDV reports personal fees as consultant or advisor for Adocia, Novo Nordisk, and Zealand. ER reports personal fees as consultant or advisor for Abbott, Air Liquide, AstraZeneca, Boehringer-Ingelheim, Cellnovo, Dexcom, Eli Lilly, Insulet, Johnson & Johnson (Animas, LifeScan), Medirio, Medtronic, Novo Nordisk, Roche Diagnostics, Sanofi-Aventis, and Tandem; and research grant or material support from Abbott, Dexcom, Insulet, Roche Diagnostics, and Tandem. BG reports personal fees as consultant or advisor for Novo Nordisk, Pfizer, Merck Sharp & Dohme, Astra Zeneca, and Takeda. FR reports personal fees as a consultant or advisor for Ethicon, Medtronic, and Novo Nordisk. All other authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
