

Clinical predictive factors for vaginal delivery following induction of labour among pregnant women in Jordan
- PMID: 34620120
- PMCID: PMC8496008
- DOI: 10.1186/s12884-021-04151-3
Clinical predictive factors for vaginal delivery following induction of labour among pregnant women in Jordan
Abstract
Background: Induction of labour (IOL) is an important and common clinical procedure in obstetrics. In the current study, we evaluate predictors of vaginal delivery in both nulliparous and multiparous women in north Jordan who were induced with vaginal prostaglandins.
Method: A prospective study was conducted on 530 pregnant women at King Abdullah University Hospital (KAUH) in north Jordan. All pregnant mothers with singleton live fetuses, who had induction of labour (IOL) between July 2017 and June 2019, were included in the study. Mode of delivery, whether vaginal or caesarean, was the primary outcome. Several maternal and fetal variables were investigated. The safety and benefit of repeated dosage of vaginal prostaglandin E2 (PGE2) tablets, neonatal outcomes and factors that affect duration of labour were also evaluated. Pearson χ2 test was used to investigate the significance of association between categorical variables, while student's t-test and ANOVA were applied to examine the mean differences between categorical and numerical variables. Linear regression analysis was utilized to study the relation between two continuous variables. A multivariate regression analysis was then performed. Significance level was considered at alpha less than 0.05.
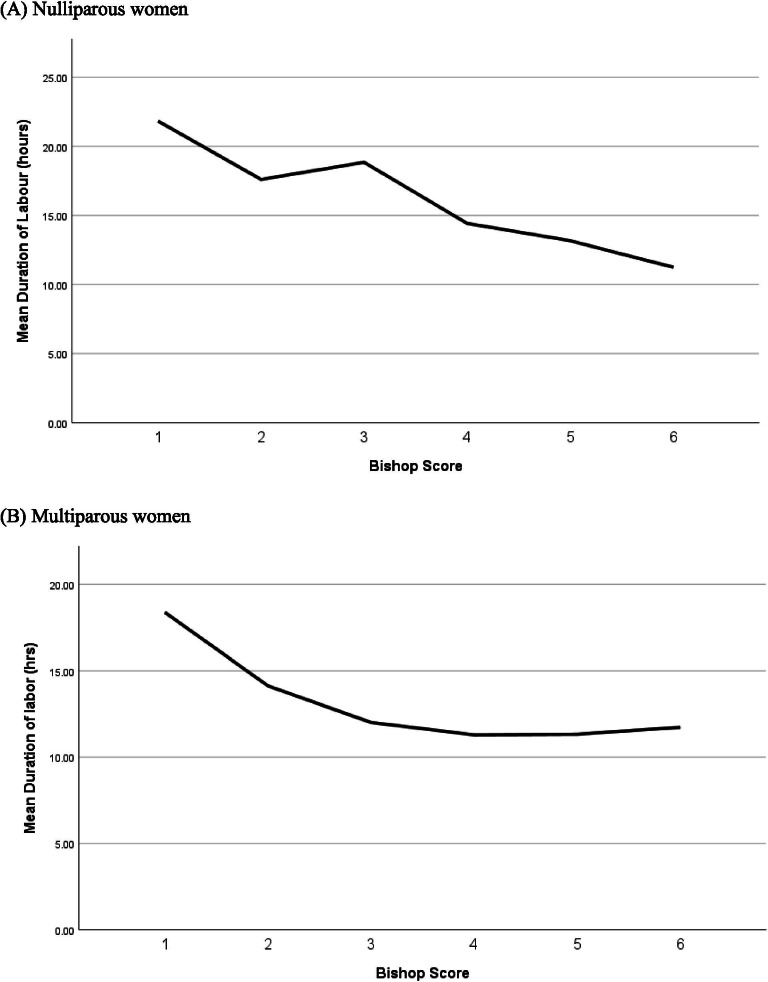
Results: Nulliparous women (N = 254) had significantly higher cesarean delivery rate (58.7% vs. 17.8%, p < 0.001) and longer duration of labour (16.1 ± 0.74 h vs. 11.0 ± 0.43 h, p < 0.001) than multiparous women (N = 276). In nulliparous women, the rate of vaginal delivery was significantly higher in women with higher Bishop score; the mean Bishop score was 3.47 ± 0.12 in nulliparous women who had vaginal delivery vs. 3.06 ± 0.10 in women who had cesarean delivery (Adjusted odds ratio (AOR) = 1.2, 95% CI: 1.03-1.28, p = 0.03). In multiparous women, the rate of vaginal delivery was significantly higher in women with higher Bishop scores and lower in women with higher body mass index (BMI). The mean Bishop score was 3.97 ± 0.07 in multiparous women who had vaginal delivery vs. 3.56 ± 0.16 in women who had cesarean delivery (AOR = 1.5, 95% CI: 1.1-2.1, p = 0.01). The mean BMI was 30.24 ± 0.28 kg/m2 in multiparous women who had vaginal delivery vs. 32.36 ± 0.73 kg/m2 in women who had cesarean delivery (AOR = 0.89, 95% CI: 0.84-0.96, p = 0.005). 27% of nulliparous women who received more than two PGE2 tablets and 50% of multiparous women who received more than two PGE2 tablets had vaginal delivery with no significant increase in neonatal morbidity.
Conclusion: Parity and cervical status are the main predictors of successful labour induction. Further studies are required to investigate the benefit of the use of additional doses of vaginal PGE2 above the recommended dose for IOL.
Keywords: Bishop score; Cesarean section; Induction of labour; Parity; Prostaglandin E2.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
