

Variations in disease burden of laryngeal cancer attributable to alcohol use and smoking in 204 countries or territories, 1990-2019
- PMID: 34620148
- PMCID: PMC8496083
- DOI: 10.1186/s12885-021-08814-4
Variations in disease burden of laryngeal cancer attributable to alcohol use and smoking in 204 countries or territories, 1990-2019
Abstract
Background: Alcohol consumption and smoking are the leading risk factors for laryngeal cancer (LC). Understanding the variations in disease burden of LC attributable to alcohol use and smoking is critical for LC prevention.
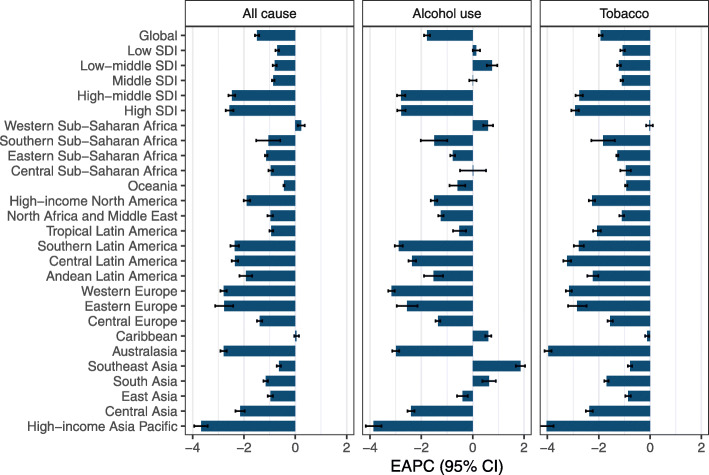
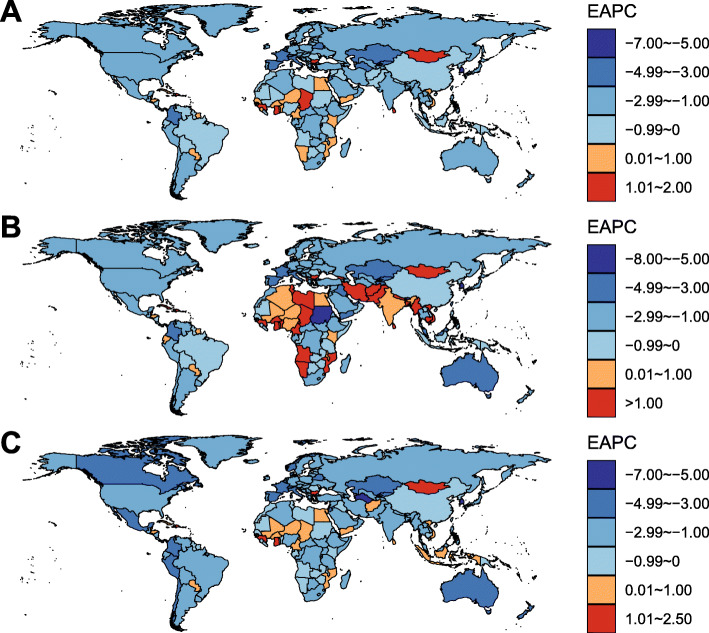
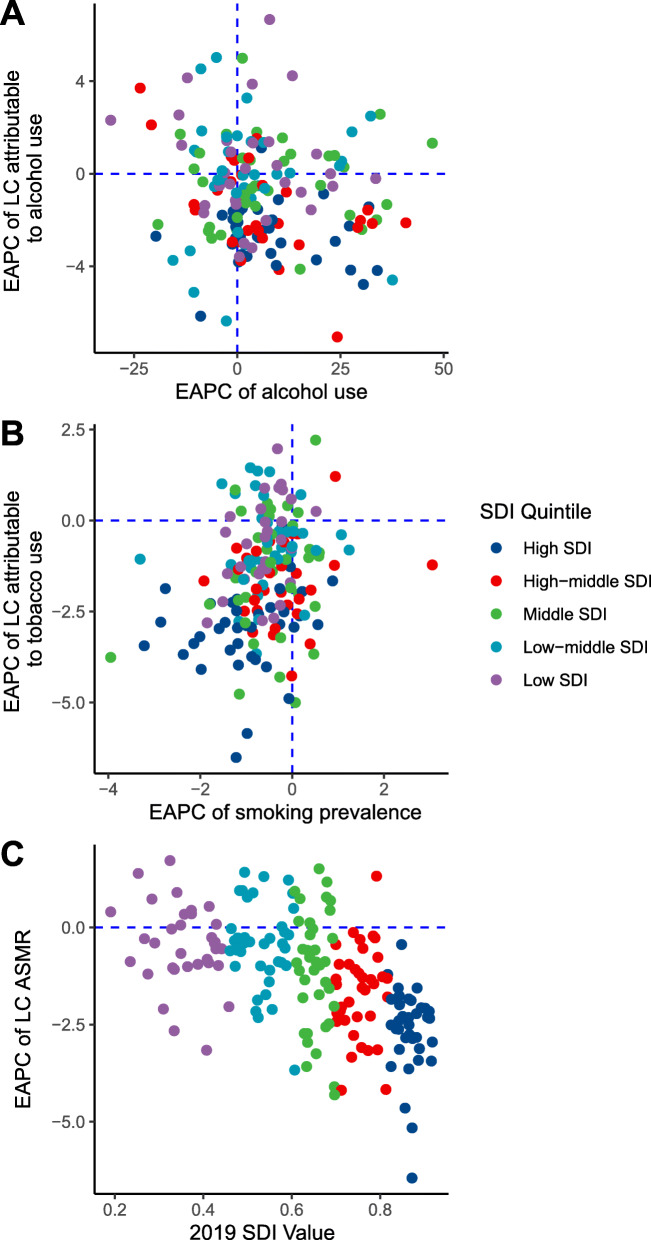
Methods: Disease burden data of LC were retrieved from the Global Burden of Disease Study 2019. We used estimated average percentage change (EAPC) to measure the temporal trends of the age-standardized mortality rate (ASMR) of LC.
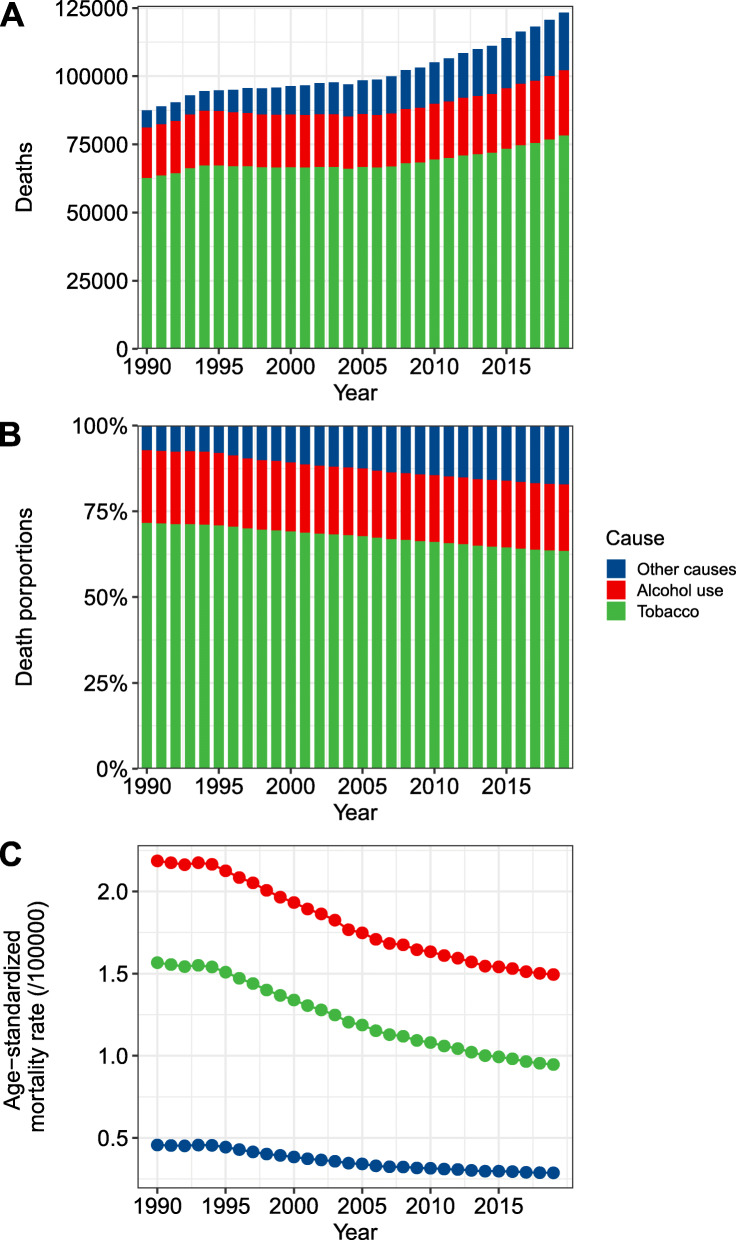
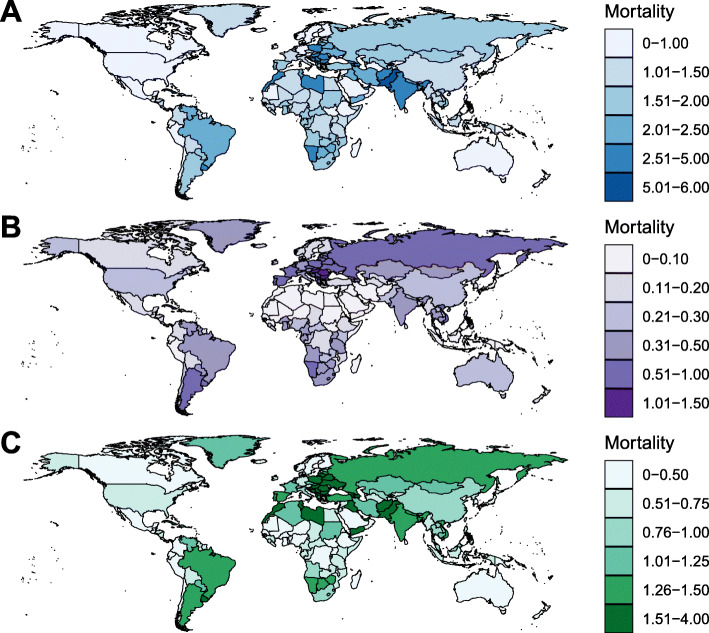
Results: Globally, while the ASMR of LC decreased by 1.49% (95% CI, 1.41-1.57%) per year between 1990 and 2019, the number of deaths from LC has increased 41.0% to 123.4 thousand in 2019. In 2019, 19.4 and 63.5% of total LC-related deaths were attributable to alcohol use and smoking worldwide, respectively. The ASMR of alcohol- and smoking-related LC decreased by 1.78 and 1.93% per year, whereas the corresponding death number has increased 29.2 and 25.1% during this period, respectively. The decreasing trend was more pronounced in developed countries. In some developing countries, such as Guinea and Mongolia, the LC mortality has shown an unfavorable trend.
Conclusion: The ubiquitous decrease in LC mortality was largely attributed to the smoking control and highlighted the importance of smoking control policies. However, the disease burden of LC remained in increase and more effective strategies are needed to combat the global increase of alcohol consumption.
Keywords: Alcohol; Disease burden; Laryngeal cancer; Mortality; Tobacco.
© 2021. The Author(s).
Conflict of interest statement
None to declare.
Figures
References
-
- Zuo JJ, Tao ZZ, Chen C, Hu ZW, Xu YX, Zheng AY, Guo Y. Characteristics of cigarette smoking without alcohol consumption and laryngeal cancer: overall and time-risk relation. A meta-analysis of observational studies. Eur Arch Otorhinolaryngol. 2017;274(3):1617–1631. doi: 10.1007/s00405-016-4390-x. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
