

sFlt-1 and CA 15.3 are indicators of endothelial damage and pulmonary fibrosis in SARS-CoV-2 infection
- PMID: 34620968
- PMCID: PMC8497540
- DOI: 10.1038/s41598-021-99470-y
sFlt-1 and CA 15.3 are indicators of endothelial damage and pulmonary fibrosis in SARS-CoV-2 infection
Abstract
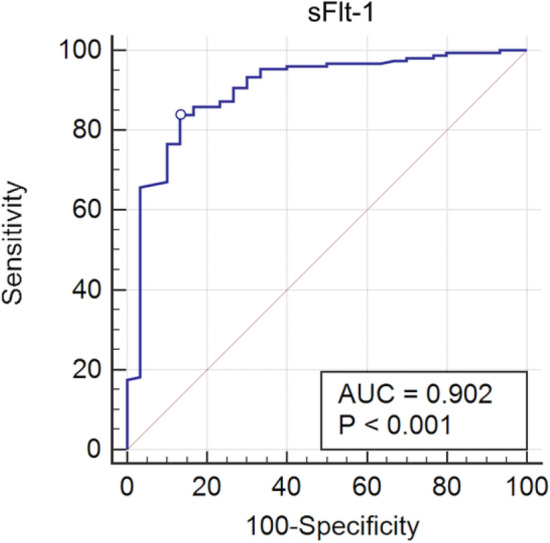
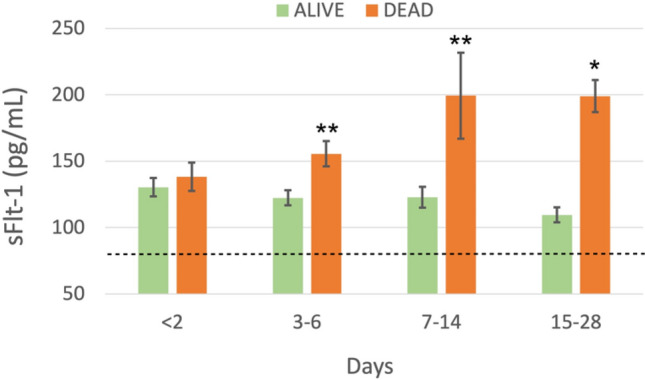
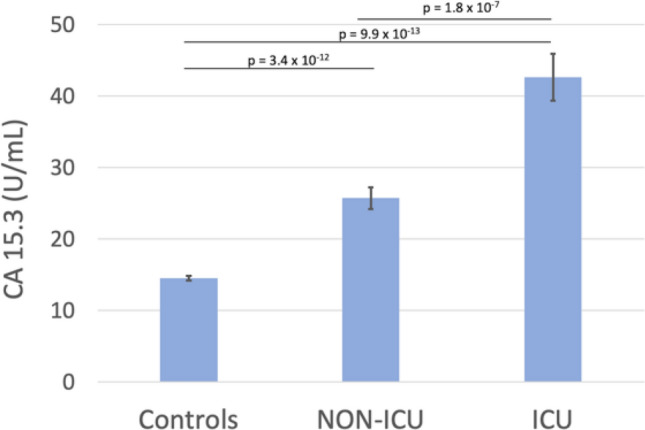
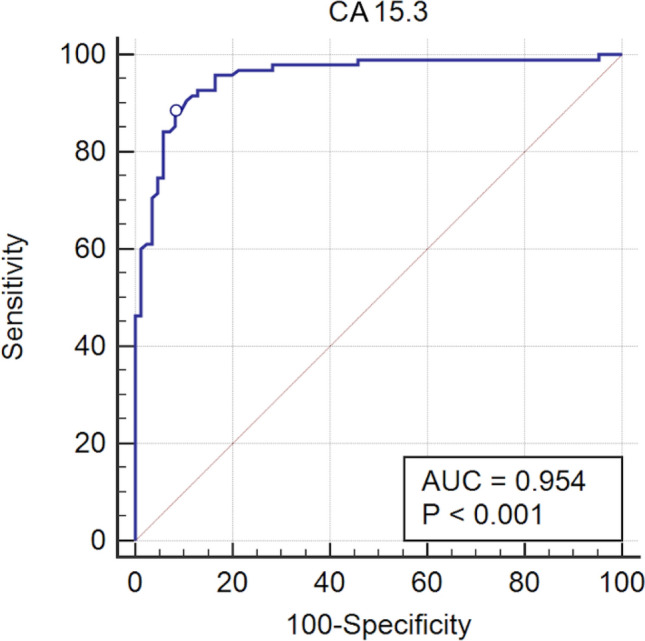
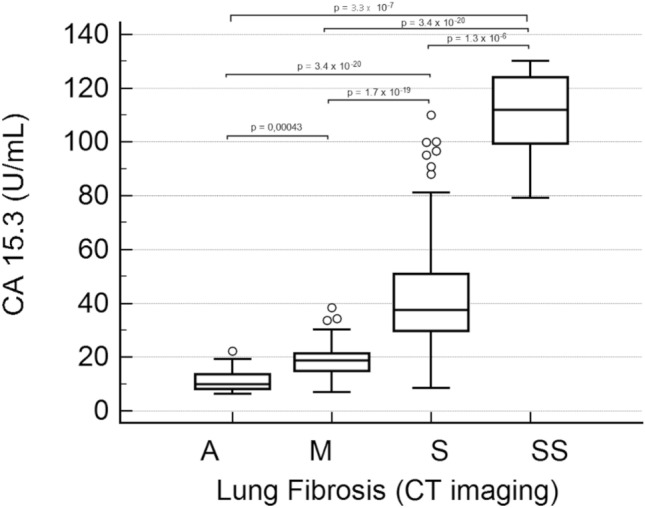
COVID-19 pandemic led to a worldwide increase of hospitalizations for interstitial pneumonia with thrombosis complications, endothelial injury and multiorgan disease. Common CT findings include lung bilateral infiltrates, bilateral ground-glass opacities and/or consolidation whilst no current laboratory parameter consents rapidly evaluation of COVID-19 risk and disease severity. In the present work we investigated the association of sFLT-1 and CA 15.3 with endothelial damage and pulmonary fibrosis. Serum sFlt-1 has been associated with endothelial injury and sepsis severity, CA 15.3 seems an alternative marker for KL-6 for fibrotic lung diseases and pulmonary interstitial damage. We analysed 262 SARS-CoV-2 patients with differing levels of clinical severity; we found an association of serum sFlt-1 (ROC AUC 0.902, decision threshold > 90.3 pg/mL, p < 0.001 Sens. 83.9% and Spec. 86.7%) with presence, extent and severity of the disease. Moreover, CA 15.3 appeared significantly increased in COVID-19 severe lung fibrosis (ICU vs NON-ICU patients 42.6 ± 3.3 vs 25.7 ± 1.5 U/mL, p < 0.0001) and was associated with lung damage severity grade (ROC AUC 0.958, decision threshold > 24.8 U/mL, p < 0.0001, Sens. 88.4% and Spec. 91.8%). In conclusion, serum levels of sFlt-1 and CA 15.3 appeared useful tools for categorizing COVID-19 clinical stage and may represent a valid aid for clinicians to better personalise treatment.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
