

Impact of Novel Guidelines on Multifactorial Control and Its Association with Mortality in Adult Patients with Hypertension and Newly Diagnosed Type 2 Diabetes: A 4-Year Prospective Multicenter Study
- PMID: 34621312
- PMCID: PMC8492251
- DOI: 10.1155/2021/9977840
Impact of Novel Guidelines on Multifactorial Control and Its Association with Mortality in Adult Patients with Hypertension and Newly Diagnosed Type 2 Diabetes: A 4-Year Prospective Multicenter Study
Abstract
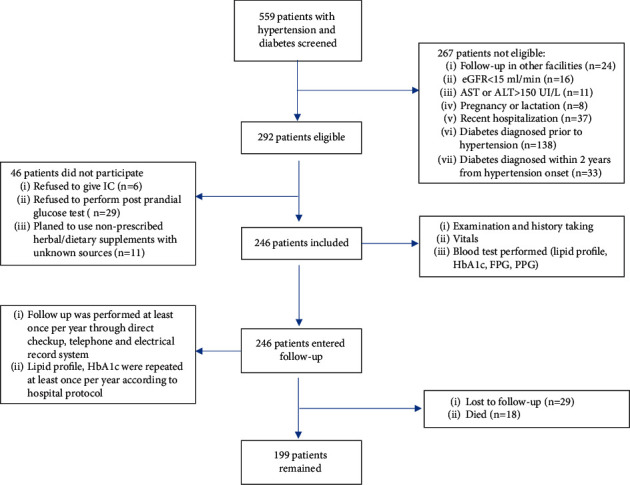
Methods: This prospective, observational study involved adult hypertensive patients with newly diagnosed type 2 diabetes mellitus at two university hospitals in Vietnam. The median time of follow-up was 4 years (August 2016-August 2020). The primary outcome was time to all-cause mortality.
Results: 246 patients were included with a mean age of 64.5 ± 10.4. 58.5% were females. 64.2% were categorized as high risk. At baseline, ischemic heart disease, dyslipidemia, and chronic kidney disease (CKD) were present in 54.9%, 67.1%, and 41.1% of patients. Renin-angiotensin-aldosterone inhibitor, metformin, and statin were prescribed in 89.8%, 66.3%, and 67.1%. Among three risk factors, LDL-c control was the hardest to achieve, increasing from 5.7% to 8.5%. In contrast, blood pressure control decreased from 56.1% in 2016 to 30.2% in 2020, when the second wave of COVID-19 hit our nation. While contemporary targets resulted in persistently low simultaneous control at 1.2%, significant improvement was observed with conventional criteria (blood pressure < 140/90 mmHg, HbA1c < 7%, LDL-c < 70 mg/dl), increasing from 14.6% to 33.7%. During follow-up, the mortality rate was 24.4 events per 1000 patient-years, exclusively in patients with early newly diagnosed diabetes. Improving control overtime, not at baseline, was associated with less mortality. Conversely, age >75 years (HR = 2.6) and CKD (HR = 4.9) were associated with increased mortality.
Conclusion: These findings demonstrated real-world difficulties in managing hypertension and newly diagnosed diabetes, especially with stringent criteria from novel guidelines. High-risk profile, high mortality, and poor simultaneous control warrant more aggressive cardiorenal protection, focusing more on aging CKD patients with early newly diagnosed diabetes.
Copyright © 2021 Ngoc-Thanh-Van Nguyen et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures





References
-
- Geldsetzer P., Manne-Goehler J., Marcus M.-E., et al. The state of hypertension care in 44 low-income and middle-income countries: a cross-sectional study of nationally representative individual-level data from 1·1 million adults. The Lancet . 2019;394(10199):652–662. doi: 10.1016/s0140-6736(19)30955-9. - DOI - PubMed
-
- Zhou B., Danaei G., Stevens G. A., Bixby H. Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: an analysis of 123 nationally representative surveys. Lancet (London, England) . 2019;394(10199):639–651. doi: 10.1016/S0140-6736(19)31145-6. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
