

Digital Quantification of Tumor PD-L1 Predicts Outcome of PD-1-Based Immune Checkpoint Therapy in Metastatic Melanoma
- PMID: 34621681
- PMCID: PMC8491983
- DOI: 10.3389/fonc.2021.741993
Digital Quantification of Tumor PD-L1 Predicts Outcome of PD-1-Based Immune Checkpoint Therapy in Metastatic Melanoma
Abstract
Background: PD-1-based immune checkpoint blockade (ICB) is a highly effective therapy in metastatic melanoma. However, 40-60% of patients are primarily resistant, with valid predictive biomarkers currently missing. This study investigated the digitally quantified tumor PD-L1 expression for ICB therapy outcome prediction.
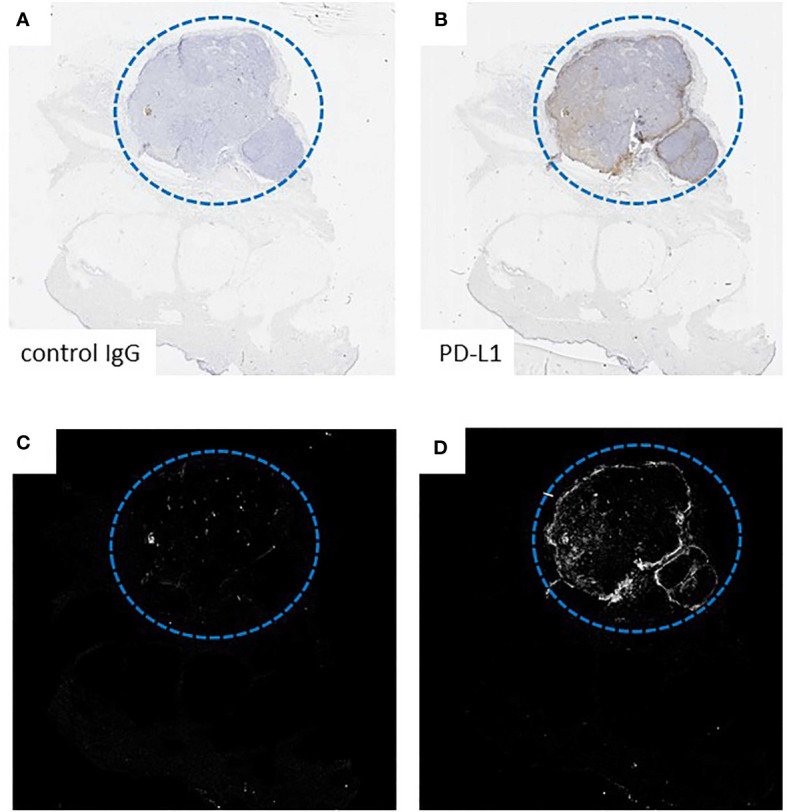
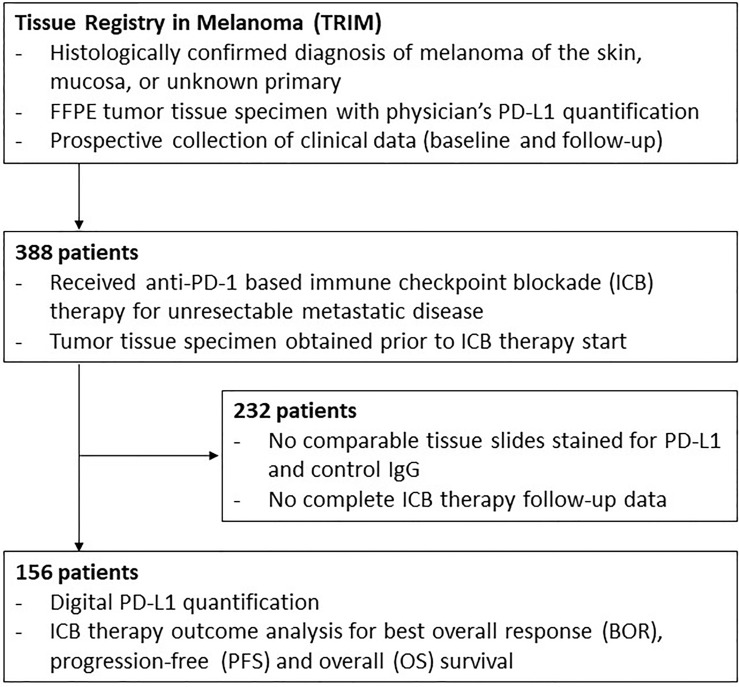
Patients and methods: Tumor tissues taken prior to PD-1-based ICB for unresectable metastatic disease were collected within the prospective multicenter Tissue Registry in Melanoma (TRIM). PD-L1 expression (clone 28-8; cut-off=5%) was determined by digital and physician quantification, and correlated with therapy outcome (best overall response, BOR; progression-free survival, PFS; overall survival, OS).
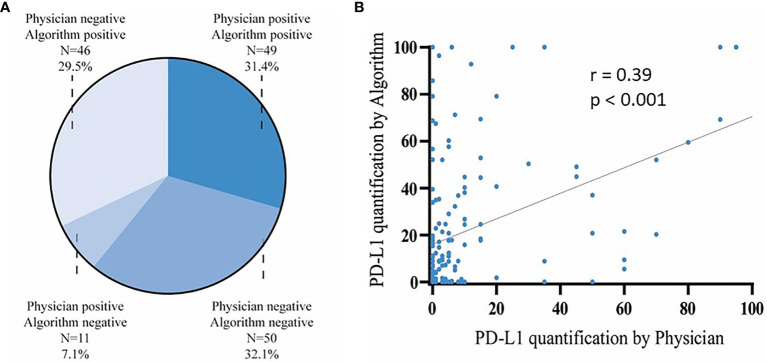
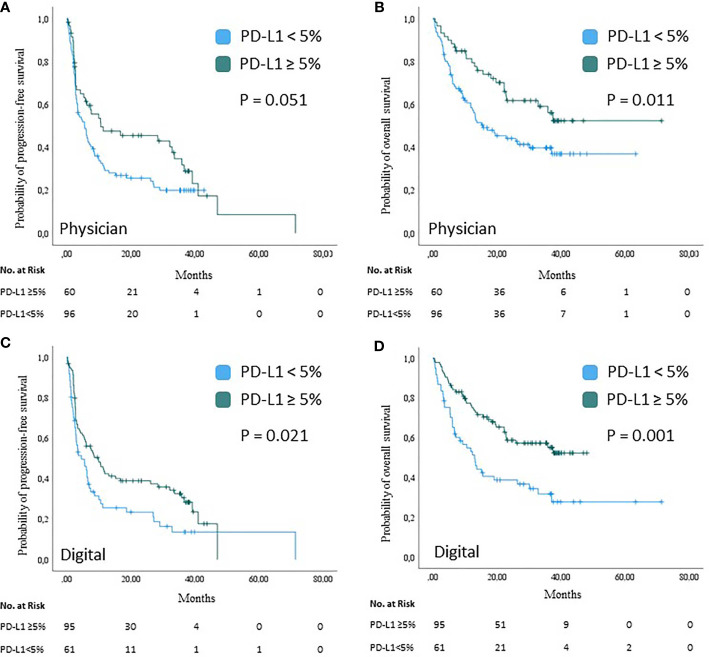
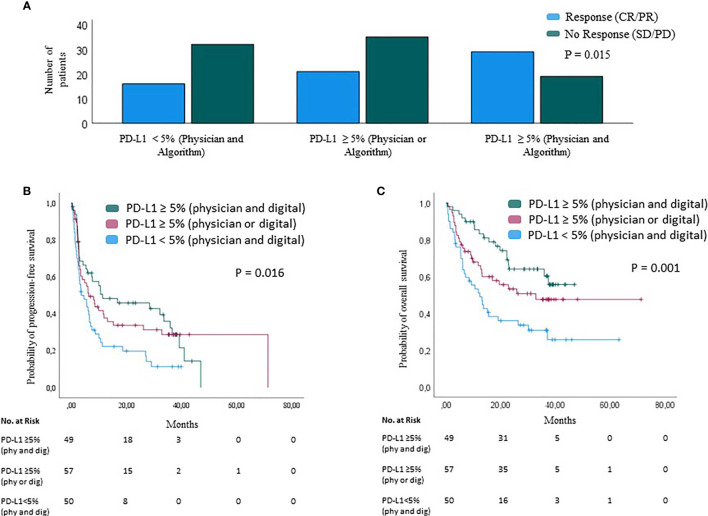
Results: Tissue samples from 156 patients were analyzed (anti-PD-1, n=115; anti-CTLA-4+anti-PD-1, n=41). Patients with PD-L1-positive tumors showed an improved response compared to patients with PD-L1-negative tumors, by digital (BOR 50.5% versus 32.2%; p=0.026) and physician (BOR 54.2% versus 36.6%; p=0.032) quantification. Tumor PD-L1 positivity was associated with a prolonged PFS and OS by either digital (PFS, 9.9 versus 4.6 months, p=0.021; OS, not reached versus 13.0 months, p=0.001) or physician (PFS, 10.6 versus 5.6 months, p=0.051; OS, not reached versus 15.6 months, p=0.011) quantification. Multivariable Cox regression revealed digital (PFS, HR=0.57, p=0.007; OS, HR=0.44, p=0.001) and physician (OS, HR=0.54, p=0.016) PD-L1 quantification as independent predictors of survival upon PD-1-based ICB. The combination of both methods identified a patient subgroup with particularly favorable therapy outcome (PFS, HR=0.53, p=0.011; OS, HR=0.47, p=0.008).
Conclusion: Pre-treatment tumor PD-L1 positivity predicted a favorable outcome of PD-1-based ICB in melanoma. Herein, digital quantification was not inferior to physician quantification, and should be further validated for clinical use.
Keywords: PD-L1 quantification; immune checkpoint blockade therapy; melanoma; response; survival.
Copyright © 2021 Placke, Soun, Bottek, Herbst, Terheyden, Utikal, Pföhler, Ulrich, Kreuter, Pfeiffer, Mohr, Gutzmer, Meier, Dippel, Weichenthal, Zimmer, Livingstone, Becker, Lodde, Sucker, Griewank, Horn, Hadaschik, Roesch, Schadendorf, Engel and Ugurel.
Conflict of interest statement
J-MP served as consultant and/or has received honoraria from Bristol-Myers Squibb, Novartis and received travel support from Bristol-Myers Squibb, Novartis and Therakos. PT declares Invited Speaker´s honoraria from Bristol-Myers Squibb, Novartis, MSD, Pierre-Fabre, CureVac, Roche, Kyowa Kirin, Biofrontera, Advisory Board honoraria from Bristol-Myers Squibb, Novartis, Pierre-Fabre, Merck Serono, Sanofi, Roche, Kyowa Kirin, and Travel support from Bristol-Myers Squibb, and Pierre-Fabre. JoU is on the advisory board or has received honoraria and travel support from Amgen, Bristol Myers Squibb, GSK, LeoPharma, Merck Sharp and Dohme, Novartis, Pierre Fabre, Roche, Sanofi outside the submitted work. ClP received honoraria (speaker honoraria or honoraria as a consultant) and travel support from: Novartis, BMS, Roche, Merck Serono, MSD, Celgene, AbbVie, AMGEN, SUNPHARMA, Allergy Therapeutics and LEO. LZ served as consultant and/or has received honoraria from Roche, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre-Fabre, and Sanofi; Research funding to institution: Novartis; travel support from Merck Sharp & Dohme, Bristol-Myers Squibb, Amgen, Pierre-Fabre, and Novartis, outside the submitted work. EL served as consultant and/or has received honoraria from Amgen, Actelion, Roche, Bris-tol-Myers Squibb, Merck Sharp & Dohme, Novartis, Janssen, Medac, Sanofi, Sunpharma and travel support from Amgen, Merck Sharp & Dohme, Bristol-Myers Squibb, Amgen, Pierre Fabre, Sunpharma and Novartis, outside the submitted work. JB is receiving speaker’s bureau honoraria from Amgen, Pfizer, MerckSerono, Recordati and Sanofi, is a paid consultant/advisory board member/DSMB member for 4SC, Almirall, Boehringer Ingelheim, ICON, InProTher, MerckSerono, Pfizer, and Sanofi/Regeneron. His group receives research grants from Merck Serono, HTG, IQVIA, and Alcedis. GL has received travel support from Sun Pharma. AR reported grants from Novartis, Bristol Myers Squibb, and Adtec; personal fees from Merck Sharp & Dohme; and nonfinancial support from Amgen, Roche, Merck Sharp & Dohme, Novartis, Bristol Myers Squibb, and Teva. DS received grants and other support from Bristol-Myers Squibb, personal fees from Bristol-Myers Squibb during the conduct of the study; personal fees from Amgen; personal fees from Boehringer Ingelheim; personal fees from InFlarX; personal fees and other support from Roche; grants, personal fees and other support from Novartis; personal fees from Incyte; personal fees and other support from Regeneron; personal fees from 4SC; personal fees from Sanofi; personal fees from Neracare; personal fees from Pierre-Fabre; personal fees and other support from Merck-EMD; personal fees from Pfizer; personal fees and other support from Philiogen; personal fees from Array, personal fees and other support from MSD Sharp & Dohme, outside the submitted work. SU declares research support from Bristol Myers Squibb and Merck Serono; speakers and advisory board honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Merck Serono, Novartis and Roche, and travel support from Bristol Myers Squibb, and Merck Sharp & Dohme. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare that this study received funding from Bristol Myers Squibb. The funder had the following involvement with the study: Financing of test material.
Figures
References
-
- Ribas A, Puzanov I, Dummer R, Schadendorf D, Hamid O, Robert C, et al. . Pembrolizumab Versus Investigator-Choice Chemotherapy for Ipilimumab-Refractory Melanoma (KEYNOTE-002): A Randomised, Controlled, Phase 2 Trial. Lancet Oncol (2015) 16:908–18. doi: 10.1016/S1470-2045(15)00083-2 - DOI - PMC - PubMed
-
- Ugurel S, Röhmel J, Ascierto PA, Becker JC, Flaherty KT, Grob JJ, et al. . Survival of Patients With Advanced Metastatic Melanoma: The Impact of MAP Kinase Pathway Inhibition and Immune Checkpoint Inhibition - Update 2019. Eur J Cancer (2020) 130:126–38. doi: 10.1016/j.ejca.2020.02.021 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials