

Pediatric temporal fistula: Report of three cases
- PMID: 34621831
- PMCID: PMC8462237
- DOI: 10.12998/wjcc.v9.i26.7811
Pediatric temporal fistula: Report of three cases
Abstract
Background: Pediatric temporal fistulae are rarely reported in the literature. Dissemination of these cases can help inform future diagnosis and effective treatment.
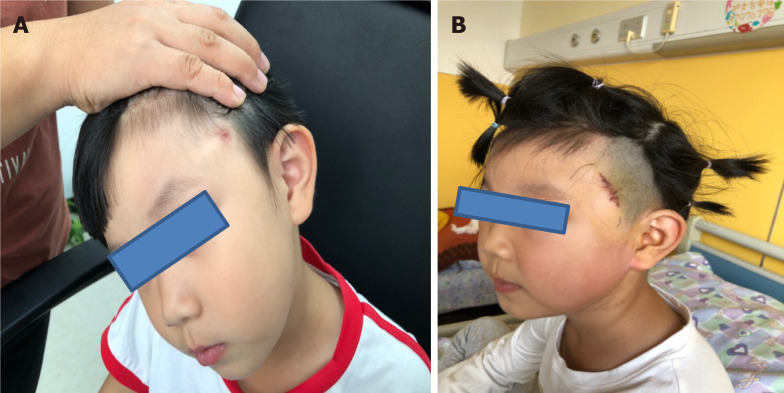
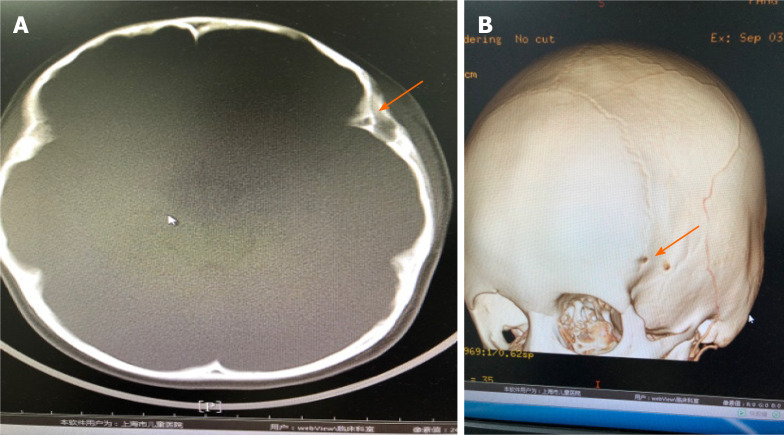
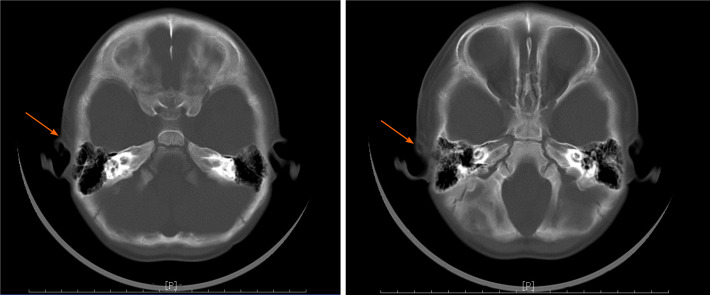
Case summary: Three pediatric patients came to the clinic due to repeated infections of the skin and soft tissue of the temporal area. One patient presented with a temporal fistula that penetrated the temporal bone and reached the dura mater. Another patient presented with a temporal fistula that penetrated into the temporal muscle fascia. The third patient presented with a fistula that penetrated the lateral wall of the orbit and entered the orbit. All patients underwent surgical fistula resection informed by preoperative computed tomography (CT) evaluation. Histopathological evaluation was also performed. All three patients were surgically treated successfully. Histopathological evaluations confirmed the fistula diagnoses in all three cases.
Conclusion: For patients who have temporal fistulae with repeated infections, surgical treatment should be performed as soon as possible to prevent serious complications. CT can be very useful for preoperative evaluation. B-mode ultrasound examination and evaluation also have a certain auxiliary role.
Keywords: Case report; Congenital; Infection; Pediatric; Surgery; Surgical treatment; Temporal fistula.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors declare no conflict of interest for this manuscript.
Figures

Similar articles
-
[Studies of labyrinthine cholesteatoma-related fistulas: report of 22 cases].J Otolaryngol. 2005 Feb;34(1):1-6. doi: 10.2310/7070.2005.00001. J Otolaryngol. 2005. PMID: 15966468 Review. French.
-
Definitive surgical management for second branchial cleft fistula: a case series.J Otolaryngol Head Neck Surg. 2020 Aug 5;49(1):55. doi: 10.1186/s40463-020-00453-2. J Otolaryngol Head Neck Surg. 2020. PMID: 32758294 Free PMC article.
-
The role of preoperative CT scan in patients with tracheoesophageal fistula: a review.J Pediatr Surg. 2013 Sep;48(9):1966-71. doi: 10.1016/j.jpedsurg.2013.06.010. J Pediatr Surg. 2013. PMID: 24074676 Review.
-
[Access for starting kidney replacement therapy: vascular and peritoneal temporal access in pre-dialysis].Nefrologia. 2008;28 Suppl 3:105-12. Nefrologia. 2008. PMID: 19018747 Spanish.
-
[Congenital coronary fistulas: the most frequent congenital coronary anomaly].Z Kardiol. 2001 Aug;90(8):535-41. doi: 10.1007/s003920170121. Z Kardiol. 2001. PMID: 11565208 German.
References
-
- Jaiswal AK, Mahapatra AK. Giant intradiploic epidermoid cysts of the skull. A report of eight cases. Br J Neurosurg. 2000;14:225–228. - PubMed
-
- Wei L, Wang R, Wang S, Jing J, Gao J, Zhang X. Diagnosis and treatment of diploic epidermoid cysts [J] Zhongguo Weichuang Shenjingwaike Zazhi . 2006;11:418–420.
-
- Bartlett SP, Lin KY, Grossman R, Katowitz J. The surgical management of orbitofacial dermoids in the pediatric patient. Plast Reconstr Surg. 1993;91:1208–1215. - PubMed
-
- Bonavolontà G, Tranfa F, de Conciliis C, Strianese D. Dermoid cysts: 16-year survey. Ophthalmic Plast Reconstr Surg. 1995;11:187–192. - PubMed
-
- Hong SW. Deep frontotemporal dermoid cyst presenting as a discharging sinus: a case report and review of literature. Br J Plast Surg. 1998;51:255–257. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
