

Metachronous mixed cellularity classical Hodgkin's lymphoma and T-cell leukemia/lymphoma: A case report
- PMID: 34621878
- PMCID: PMC8462207
- DOI: 10.12998/wjcc.v9.i27.8177
Metachronous mixed cellularity classical Hodgkin's lymphoma and T-cell leukemia/lymphoma: A case report
Abstract
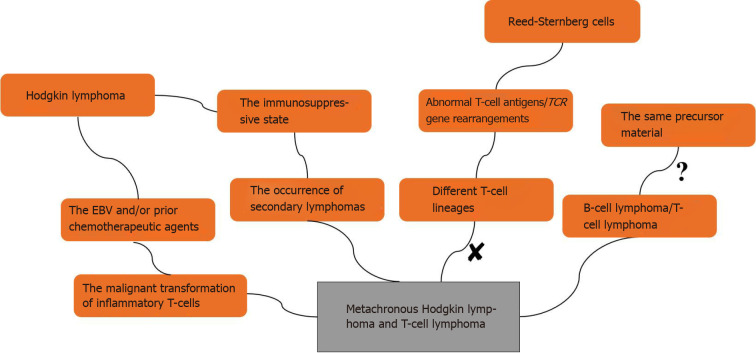
Background: The development of peripheral T-cell lymphoma (PTCL) after chemotherapy for Hodgkin's lymphoma (HL) is rare, and highly aggressive TCL/leukemia has not been reported to date. The relationship between HL and PTCL needs further exploration to understand the pathogenesis of metachronous lymphoma (ML) and find effective treatment options. We report a patient with ML, whose biopsy of a right cervical lymph node initially confirmed classical HL (CHL).
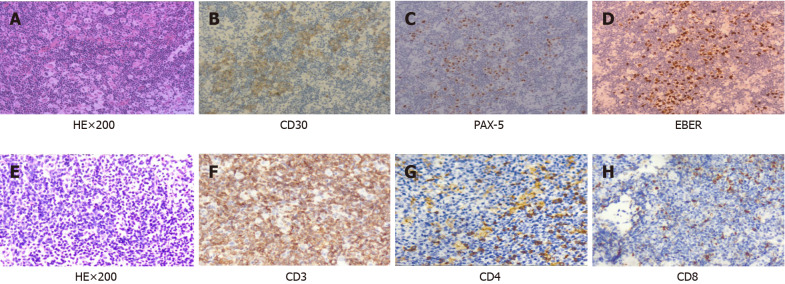
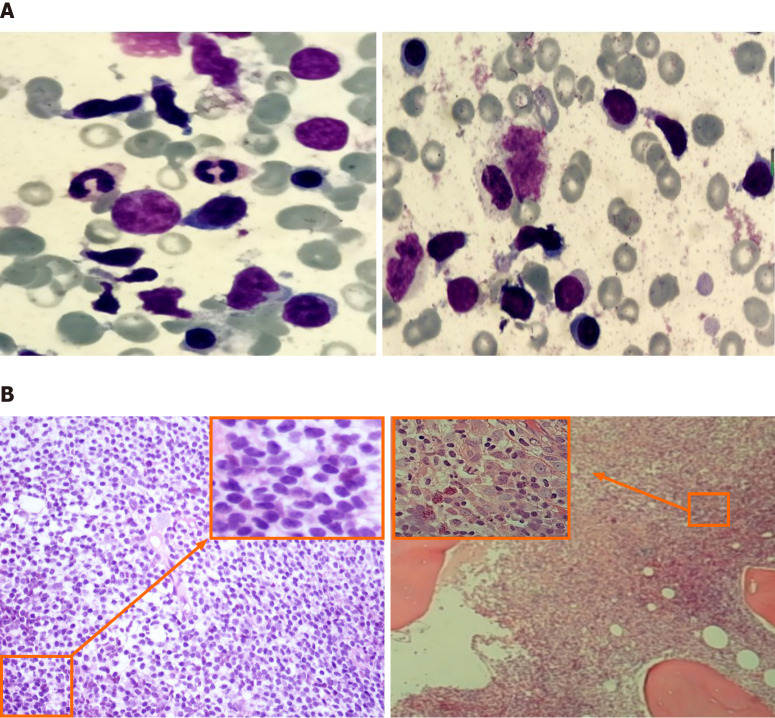
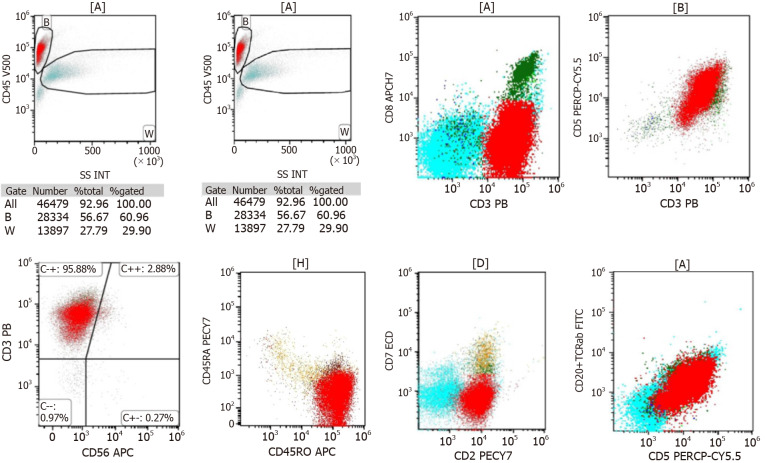
Case summary: We report a patient with ML, whose biopsy of a right cervical lymph node initially confirmed CHL, with typical reed-sternberg cells expressing CD30 and PAX-5. T-cell leukemia/lymphoma occurred 3 years after treatment, and a lymph node biopsy at the onset confirmed PTCL, nonspecific type, expressing CD3, CD4 and CD8. The patient was treated with standard doses of chemotherapy, programmed cell death-ligand 1 monoclonal antibody, and chidamide, all of which failed to achieve complete remission. The patient was diagnosed with refractory state, and eventually died of leukocyte stasis.
Conclusion: The accuracy of the diagnosis needs to be confirmed when chemotherapeutic drugs are not effective.
Keywords: Bone marrow; Case report; Chemotherapy; Classical Hodgkin’s lymphoma; Drug resistance; T-cell lymphoma/leukemia.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors do not have any possible conflicts of interest.
Figures
Similar articles
-
Peripheral T Cell Non-Hodgkin's Lymphoma following Treatment of Hodgkin's Lymphoma.Case Rep Oncol Med. 2015;2015:438385. doi: 10.1155/2015/438385. Epub 2015 Jan 13. Case Rep Oncol Med. 2015. PMID: 25664194 Free PMC article.
-
Discordant lymphocyte-depleted classical Hodgkin's and peripheral T-cell lymphoma arising in a patient 11 years after diagnosis of multicentric Castleman's disease.Int J Hematol. 2013 Jul;98(1):114-21. doi: 10.1007/s12185-013-1358-0. Epub 2013 Jun 4. Int J Hematol. 2013. PMID: 23733446
-
Peripheral T-Cell Lymphoma Following Treatment of Hodgkin Lymphoma: Report of One Case and Literature Review.Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2024 Dec;46(6):965-969. doi: 10.3881/j.issn.1000-503X.15920. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2024. PMID: 39773516 Review.
-
Expression of lymphoid-associated antigens on Hodgkin's and Reed-Sternberg cells of Hodgkin's disease. An immunocytochemical study on lymph node cytospins using monoclonal antibodies.Histopathology. 1987 Dec;11(12):1229-42. doi: 10.1111/j.1365-2559.1987.tb01869.x. Histopathology. 1987. PMID: 2831131
-
[WHO classification of Hodgkin's lymphoma and its molecular pathological relevance].Pathologe. 2002 May;23(3):207-18. doi: 10.1007/s00292-002-0529-1. Pathologe. 2002. PMID: 12089788 Review. German.
References
-
- Custer R. Pitfallsin the diagnosis of lymphoma and leukemia from the pathologist′s point of view. New York: American Cancer Society, 1954: 35-37.
-
- Geladari E, Dimopoulou G, Margellou E, Paraskevas A, Kafetzis G, Rontogianni D, Vadiaka M. Coexistence of Hodgkin and Non-Hodgkin Lymphoma; Composite Lymphoma [CL] in a Patient Presenting with Waxing and Waning Lymphadenopathy. Cardiovasc Hematol Disord Drug Targets. 2020;20:160–163. - PubMed
-
- Younes A, Hilden P, Coiffier B, Hagenbeek A, Salles G, Wilson W, Seymour JF, Kelly K, Gribben J, Pfreunschuh M, Morschhauser F, Schoder H, Zelenetz AD, Rademaker J, Advani R, Valente N, Fortpied C, Witzig TE, Sehn LH, Engert A, Fisher RI, Zinzani PL, Federico M, Hutchings M, Bollard C, Trneny M, Elsayed YA, Tobinai K, Abramson JS, Fowler N, Goy A, Smith M, Ansell S, Kuruvilla J, Dreyling M, Thieblemont C, Little RF, Aurer I, Van Oers MHJ, Takeshita K, Gopal A, Rule S, de Vos S, Kloos I, Kaminski MS, Meignan M, Schwartz LH, Leonard JP, Schuster SJ, Seshan VE. International Working Group consensus response evaluation criteria in lymphoma (RECIL 2017) Ann Oncol. 2017;28:1436–1447. - PMC - PubMed
-
- Boyer DF, Lindeman NI, Harris NL, Ferry JA. Peripheral T-cell lymphomas with cytotoxic phenotype in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma. Am J Surg Pathol. 2014;38:279–288. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
