

Major Bleeding of Transjugular Native Kidney Biopsies. A French Nationwide Cohort Study
- PMID: 34622099
- PMCID: PMC8484497
- DOI: 10.1016/j.ekir.2021.07.011
Major Bleeding of Transjugular Native Kidney Biopsies. A French Nationwide Cohort Study
Abstract
Introduction: The risk of bleeding associated with transjugular kidney biopsies is unclear, and which patients are the best candidates for this route is unknown.
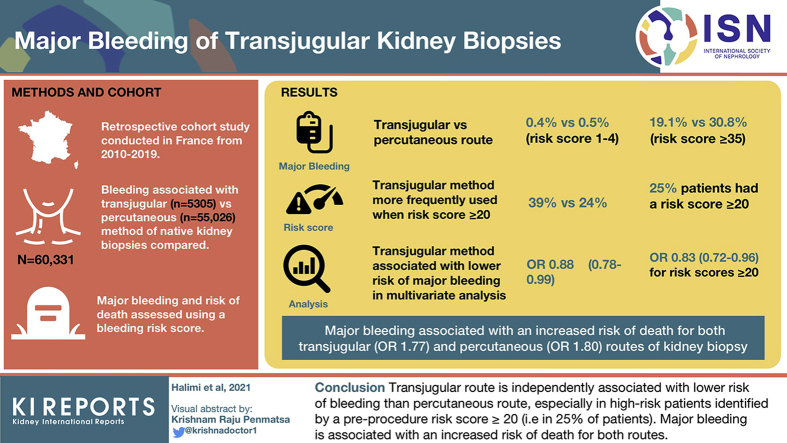
Methods: This was a retrospective cohort study comparing proportion of bleeding associated with transjugular versus percutaneous native kidney biopsies in all patients in France in the 2010-2019 period. Major bleeding at day 8 (i.e., blood transfusions, hemorrhage/hematoma, angiographic intervention, nephrectomy) and risk of death at day 30 were assessed, and we used a bleeding risk score initially developed for the percutaneous route.
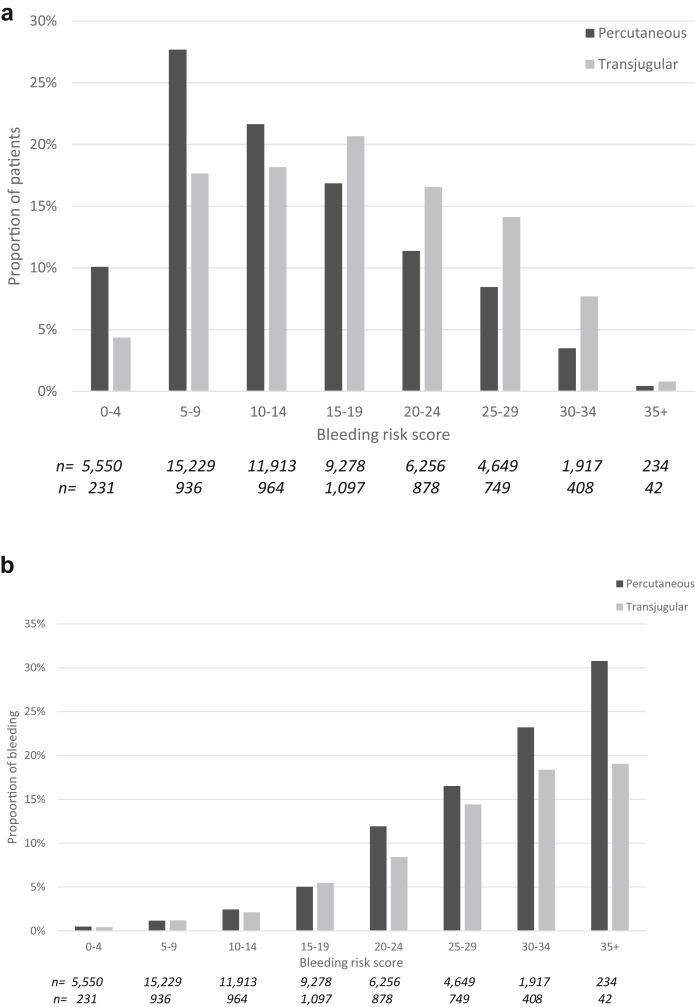
Results: Our analysis included 60,331 patients (transjugular route: 5305; percutaneous route: 55,026 patients). The observed proportion of major bleeding varied widely (transjugular vs. percutaneous): 0.4% versus 0.5% for the lowest risk scores (0-4) to 19.1% versus 30.8% for the highest risk scores (≥35). Transjugular was more frequently used than percutaneous route (39% vs. 24%) when the risk score was ≥20 (15,133/60,331; 25% of all patients). Transjugular was associated with a lower risk of major bleeding than percutaneous route in multivariate analyses (odds ratio [OR]: 0.88 [0.78-0.99]), especially for scores ≥20 (OR: 0.83 [0.72-0.96], (i.e., 25% of patients). Major bleeding was associated with an increased risk of death both for transjugular (OR: 1.77 [1.00-3.14]) and percutaneous (OR: 1.80 [1.43-2.28]) routes.
Conclusions: The transjugular route is independently associated with a lower risk of bleeding than the percutaneous route, especially in high-risk patients identified by a preprocedure risk score ≥20 (i.e., 25% of patients). Major bleeding is associated with an increased risk of death for both routes.
Keywords: bleeding score; epidemiology; kidney biopsy; percutaneous; transjugular.
© 2021 Published by Elsevier, Inc., on behalf of the International Society of Nephrology.
Figures

References
-
- Mal F., Meyrier A., Callard P. Transjugular renal biopsy. Lancet. 1990;335:1512–1513. - PubMed
-
- Cluzel P., Martinez F., Bellin M.F. Transjugular versus percutaneous renal biopsy for the diagnosis of parenchymal disease: comparison of sampling effectiveness and complications. Radiology. 2000;215(3):689–693. - PubMed
-
- Nielly H., Mathian A., Cazenave M. Safety and effectiveness of transjugular renal biopsy for systemic lupus erythematosus and antiphospholipid antibody syndrome patients taking antithrombotics. Nephrol Dial Transplant. 2020;35:1721–1729. - PubMed
LinkOut - more resources
Full Text Sources
