

An Integrated Pharmacokinetic-Pharmacodynamic-Pharmacoeconomic Modeling Method to Evaluate Treatments for Adults with Schizophrenia
- PMID: 34622429
- PMCID: PMC8738623
- DOI: 10.1007/s40273-021-01077-8
An Integrated Pharmacokinetic-Pharmacodynamic-Pharmacoeconomic Modeling Method to Evaluate Treatments for Adults with Schizophrenia
Abstract
Introduction: Schizophrenia is a chronic mental disorder that worsens with each relapse. Long-acting injectable (LAI) antipsychotics may prevent the exacerbation of symptoms and occurrence of relapses through improved continuity of care. Different dose regimens are available for the LAIs aripiprazole monohydrate (AM) and aripiprazole lauroxil (AL), but their cost effectiveness is unclear.
Objectives: The study aim was to compare costs and effects (relapses) of the different aripiprazole LAI dose regimens to inform clinical and US payer decisions.
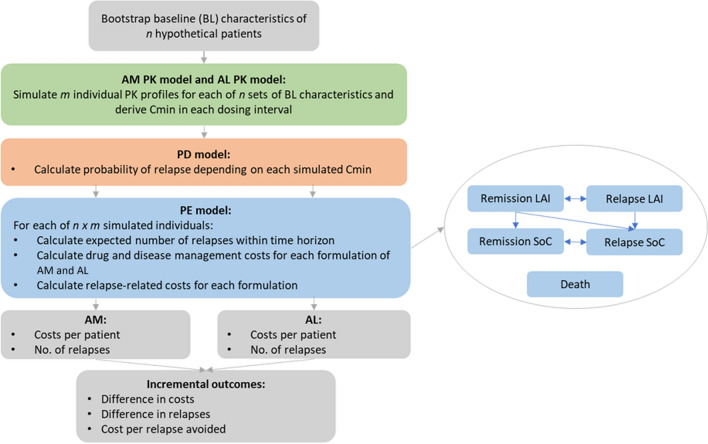
Methods: A state-transition model calculated the outcomes of eight LAI dose regimens based on their relapse rates. As effectiveness data from randomized controlled trials were unavailable, relapse rates were modeled using pharmacokinetic and pharmacodynamic evidence. These described blood plasma levels of aripiprazole as a function of AM and AL dose regimens and described the probability of relapse as a function of aripiprazole blood plasma levels. The analysis had a time horizon of 1 year and took the US healthcare payer perspective. The incremental cost per relapse avoided and the probability of cost effectiveness were calculated in deterministic and probabilistic analyses. Scenario analyses explored the model's main assumptions, and results were validated against external data and other cost-effectiveness analyses.
Results: Monthly administration of AM 400 mg consistently yielded the lowest predicted number of relapses across deterministic, probabilistic, and scenario analyses. The costs of treatment and relapses were projected to be the lowest with a monthly administration of AL 441 mg. The incremental cost per relapse avoided with AM 400 mg ranged from AM 400 mg being dominant to $US83,300. From willingness-to-pay thresholds of $US30,000 per relapse avoided, the probability of cost effectiveness was highest for AM 400 mg. The validation showed alignment with external data.
Conclusion: The analysis highlighted the robustness of the novel framework based on pharmacokinetic and pharmacodynamic evidence and demonstrated an application in a postmarketing setting.
© 2021. The Author(s).
Conflict of interest statement
MAP, NH, CB, and CK are employees of OPEN Health and were paid consultants to Otsuka with regard to the development of this manuscript. HW, RAD, XW, and SM are employees of Otsuka. MAP, NH, CB, CK, HW, RAD, XW, and SM have no conflicts of interest that are directly relevant to the content of this article.
Figures


Comment in
-
Response to Comment on "An Integrated Pharmacokinetic-Pharmacodynamic-Pharmacoeconomic Modeling Method to Evaluate Treatments for Adults with Schizophrenia".Pharmacoeconomics. 2022 Dec;40(12):1265-1267. doi: 10.1007/s40273-022-01213-y. Epub 2022 Nov 11. Pharmacoeconomics. 2022. PMID: 36357767 Free PMC article. No abstract available.
-
Comment on "An Integrated Pharmacokinetic-Pharmacodynamic-Pharmacoeconomic Modeling Method to Evaluate Treatments for Adults with Schizophrenia".Pharmacoeconomics. 2022 Dec;40(12):1261-1263. doi: 10.1007/s40273-022-01200-3. Epub 2022 Nov 11. Pharmacoeconomics. 2022. PMID: 36357768 Free PMC article. No abstract available.
References
-
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria; 2020. http://www.R-project.org/.
-
- National Collaborating Centre for Mental Health. Schizophrenia: core interventions in the treatment and management of schizophrenia in primary and secondary care (Update). Leicester (UK): British Psychological Society. Copyright©. 2009. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
