

Cardiovascular Diseases That Have Emerged From the Darkness
- PMID: 34622668
- PMCID: PMC8751898
- DOI: 10.1161/JAHA.121.021095
Cardiovascular Diseases That Have Emerged From the Darkness
Abstract
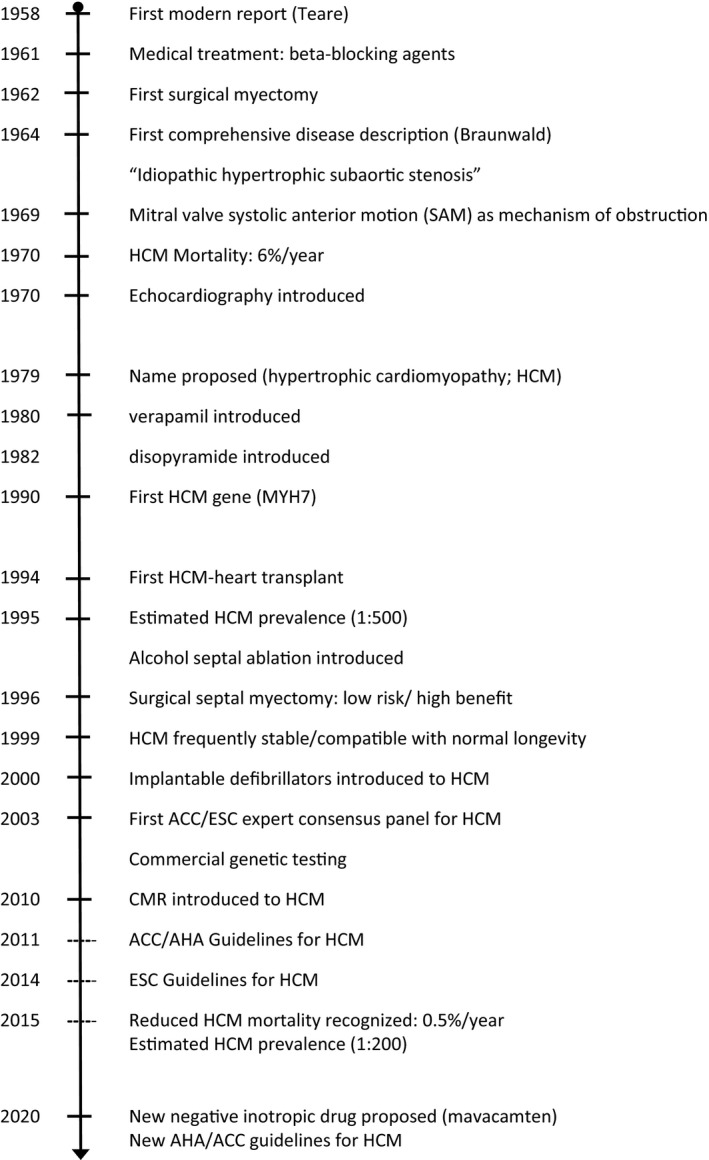
It is important for both the patient and physician communities to have timely access to information recognizing rapid progress in the diagnosis and treatment of familiar but relatively uncommon cardiovascular diseases. Patients with 3 cardiovascular diseases (ie, hypertrophic cardiomyopathy, pulmonary arterial hypertension, and transthyretin (TTR) cardiac amyloidosis (ATTR)]), once considered rare without effective management options and associated with malignant prognosis, have now benefited substantially from the development of a variety of innovative therapeutic strategies. In addition, in each case, enhanced diagnostic testing has expanded the patient population and allowed for more widespread administration of contemporary treatments. In hypertrophic cardiomyopathy, introduction of implantable defibrillators to prevent sudden death as well as high-benefit:low-risk septal reduction therapies to reverse heart failure have substantially reduced morbidity and disease-related mortality (to 0.5% per year). For pulmonary arterial hypertension, a disease once characterized by a particularly grim prognosis, prospective randomized drug trials with aggressive single (or combined) pharmacotherapy have measurably improved survival and quality of life for many patients. In cardiac amyloidosis, development of disease-specific drugs can for the first time reduce morbidity and mortality, prominently with breakthrough ATTR-protein-stabilizing tafamidis. In conclusion, in less common and visible cardiovascular diseases, it is crucial to recognize substantial progress and achievement, given that penetration of such information into clinical practice and the patient community can be inconsistent. Diseases such as hypertrophic cardiomyopathy, pulmonary arterial hypertension, and ATTR cardiac amyloidosis, once linked to a uniformly adverse prognosis, are now associated with the opportunity for patients to experience satisfactory quality of life and extended longevity.
Keywords: amyloid; drug therapy; heart failure; hypertrophic cardiomyopathy; implantable cardioverter‐defibrillator; pulmonary hypertension; sudden death.
Conflict of interest statement
Dr B.A. Maron reports consulting for Actelion Pharmaceuticals. Dr Rowin reports a research grant from Pfizer. Dr M.S. Maron is a Steering Committee member for Cytokinetics and a consultant for Imbria pharmaceuticals. Dr Mauer reports research support from the National Institutes of Health (R01HL139671‐01, R21AG058348, K24AG036778); has consulted for Pfizer, GSK, Intellia, Eldos, Prothena, Akcea and Alnylam; and has received institutional clinical trial funding from Pfizer, Prothena, Eidos, and Alnylam. Dr Galiè is on the following Advisory Boards: Actelion, Janssen, Pfizer, Ferrer, and reports research grants from Janssen and paid lectures for Actelion, Janssen, Pfizer, and Ferrer. Dr B.J. Maron has no disclosures to report.
Figures






References
-
- Maron BJ, Shen W‐K, Link MS, Epstein AE, Almquist AK, Daubert JP, Bardy GH, Favale S, Rea RF, Boriani G, et al. Efficacy of implantable cardioverter‐defibrillators for the prevention of sudden death in patients with hypertrophic cardiomyopathy. N Engl J Med. 2000;342:365–373. DOI: 10.1056/NEJM200002103420601. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
