

The lymphocyte/monocyte ratio and red blood cell transfusion during radical retropubic prostatectomy
- PMID: 34623495
- PMCID: PMC8497187
- DOI: 10.1007/s00540-021-03008-5
The lymphocyte/monocyte ratio and red blood cell transfusion during radical retropubic prostatectomy
Abstract
Purpose: Despite improvements of strategy in radical retropubic prostatectomy, blood loss is still a major concern. The lymphocyte/monocyte (LM) ratio is a prognostic indicator for various diseases. We identified the risk factors, including the LM ratio, for red blood cell (RBC) transfusion during radical retropubic prostatectomy.
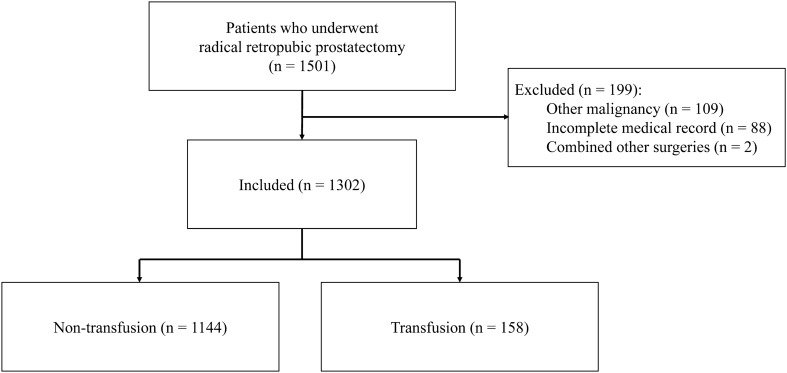
Methods: This retrospective study assessed patients who underwent radical retropubic prostatectomy between March 2009 and December 2020. To determine the risk factors for RBC transfusion, a multivariate logistic regression analysis was conducted. A receiver operating characteristic (ROC) curve analysis was also performed. Postoperative outcomes, including acute kidney injury (AKI), hospitalization duration, and intensive care unit (ICU) admission, were also evaluated.
Results: Among 1302 patients, 158 patients (12.1%) received an intraoperative RBC transfusion. Multivariate logistic regression analysis demonstrated that the risk factors for RBC transfusion were the LM ratio, hemoglobin, 6% hydroxyethyl starch amount, and positive surgical margin. The area under the ROC curve of LM ratio was 0.706 (cut-off = 4.3). The LM ratio at ≤ 4.3 was significantly related to transfusion in multivariate-adjusted analysis (odds ratio = 4.598, P < 0.001). AKI and ICU admission were significantly higher, and the hospitalization duration was significantly longer in patients with RBC transfusion.
Conclusions: The LM ratio was a risk factor for RBC transfusion in radical retropubic prostatectomy. The optimal cut-off value of the LM ratio to predict transfusion was 4.3. RBC transfusion was associated with poor postoperative outcomes. Therefore, our results suggest that the LM ratio provide useful information on RBC transfusion in radical retropubic prostatectomy.
Keywords: Acute kidney injury; Hospitalization duration; Intensive care unit admission; Lymphocyte/monocyte ratio; Radical retropubic prostatectomy; Transfusion.
© 2021. Japanese Society of Anesthesiologists.
Conflict of interest statement
The authors have no conflicts of interest.
Figures


References
-
- Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, Fossati N, Gross T, Henry AM, Joniau S, Lam TB, Mason MD, Matveev VB, Moldovan PC, van den Bergh RCN, Van den Broeck T, van der Poel HG, van der Kwast TH, Rouvière O, Schoots IG, Wiegel T, Cornford P. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2017;71(4):618–29. doi: 10.1016/j.eururo.2016.08.003. - DOI - PubMed
-
- Gainsburg DM. Anesthetic concerns for robotic-assisted laparoscopic radical prostatectomy. Minerva Anestesiol. 2012;78(5):596–604. - PubMed
-
- Kordan Y, Barocas DA, Altamar HO, Clark PE, Chang SS, Davis R, Herrell SD, Baumgartner R, Mishra V, Chan RC, Smith JA, Jr, Cookson MS. Comparison of transfusion requirements between open and robotic-assisted laparoscopic radical prostatectomy. BJU Int. 2010;106(7):1036–1040. doi: 10.1111/j.1464-410X.2010.09233.x. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
