

Hallmarks of response, resistance, and toxicity to immune checkpoint blockade
- PMID: 34624224
- PMCID: PMC8767569
- DOI: 10.1016/j.cell.2021.09.020
Hallmarks of response, resistance, and toxicity to immune checkpoint blockade
Erratum in
-
Hallmarks of response, resistance, and toxicity to immune checkpoint blockade.Cell. 2022 Feb 3;185(3):576. doi: 10.1016/j.cell.2022.01.008. Cell. 2022. PMID: 35120665 No abstract available.
Abstract
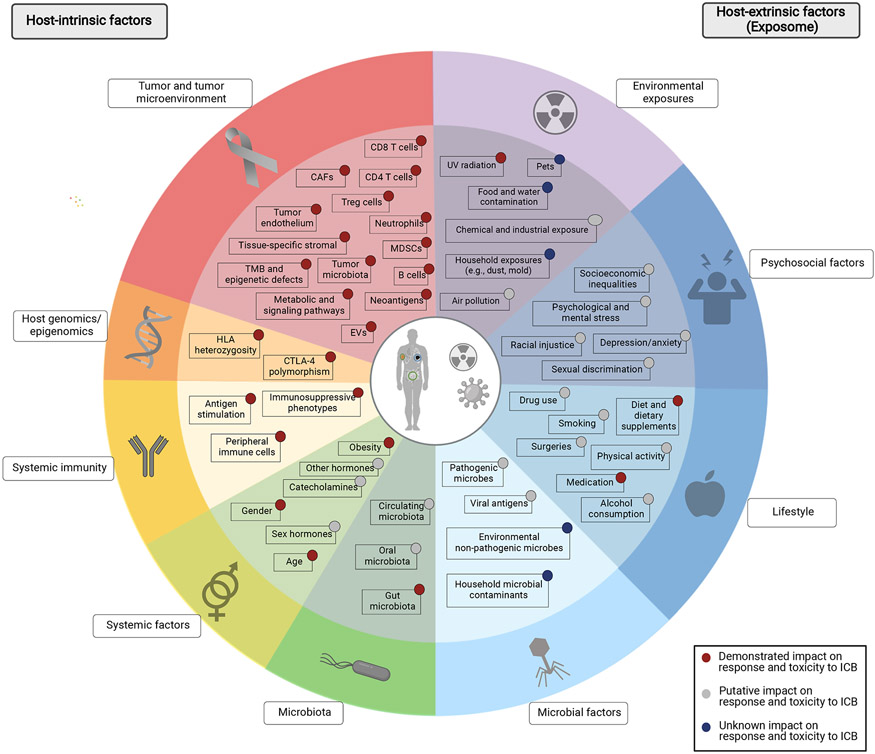
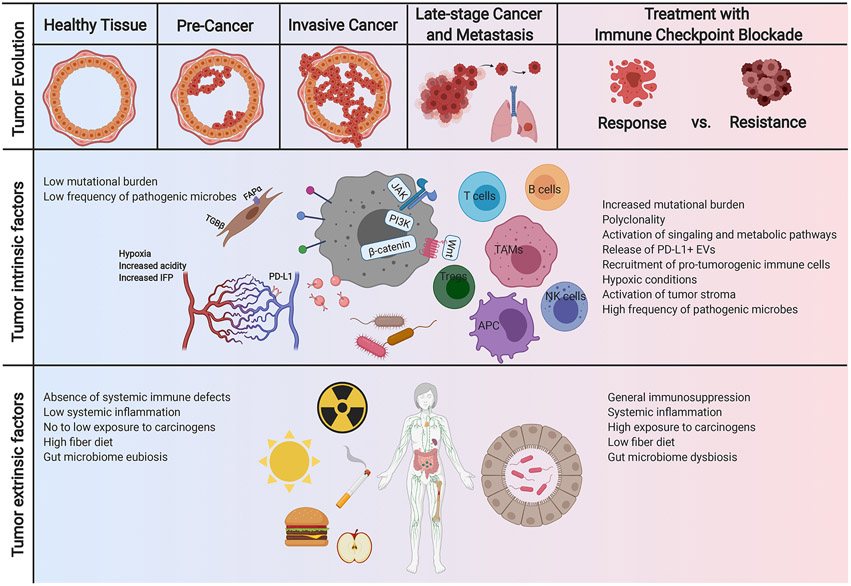
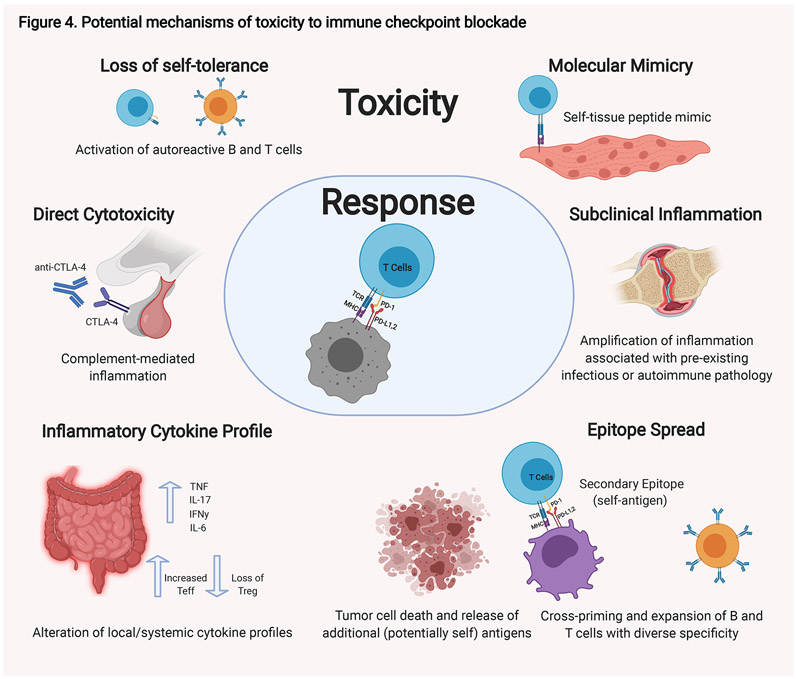
Unprecedented advances have been made in cancer treatment with the use of immune checkpoint blockade (ICB). However, responses are limited to a subset of patients, and immune-related adverse events (irAEs) can be problematic, requiring treatment discontinuation. Iterative insights into factors intrinsic and extrinsic to the host that impact ICB response and toxicity are critically needed. Our understanding of the impact of host-intrinsic factors (such as the host genome, epigenome, and immunity) has evolved substantially over the past decade, with greater insights on these factors and on tumor and immune co-evolution. Additionally, we are beginning to understand the impact of acute and cumulative exposures-both internal and external to the host (i.e., the exposome)-on host physiology and response to treatment. Together these represent the current day hallmarks of response, resistance, and toxicity to ICB. Opportunities built on these hallmarks are duly warranted.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests B.A.H. reports no conflicts of interest. G.M. is a co-inventor on US patents (PCT/US2019/022194, PCT/US2020/029556, PCT/US2020/046050) relating to extracellular vesicles. P.S. reports consulting, advisory roles, and/or stocks/ownership for Achelois, Adaptive Biotechnologies, Apricity Health, BioAlta, BioNTech, Codiak Biosciences, Constellation, Dragonfly Therapeutics, Forty-Seven Inc., Hummingbird, ImaginAb, Infinity Pharma, Jounce Therapeutics, Lave Therapeutics, Lytix Biopharma, Marker Therapeutics, Oncolytics, Phenomics, and Polaris Pharma and owns a patent licensed to Jounce Therapeutics. P.S. reports consulting, stock ownership, or advisory board membership for Achelois, Adaptive Biotechnologies, Apricity, BioAtla, BioNTech, Candel Therapeutics, Codiak, Dragonfly, Earli, Enable Medicine, Hummingbird, ImaginAb, Jounce, Lava Therapeutics, Lytix, Marker, PBM Capital, Phenomic AI, Polaris Pharma, Time Bioventures, and Trained Therapeutix and Venn Biosciences for an immediate family member. J.A.W. is a co-inventor on a US patent (PCT/US17/53,717) relating to the microbiome. J.A.W. reports speaker fees from Imedex, Dava Oncology, Omniprex, Illumina, Gilead, MedImmune, and BMS; consultant/advisor roles or advisory board membership for Roche-Genentech, Novartis, AstraZeneca, GSK, BMS, Merck/MSD, Biothera Pharma, and Microbiome DX; and receives clinical trial support from GSK, Roche-Genentech, BMS, and Novartis, all outside the current work.
Figures
References
-
- Abu-Sbeih H, and Wang Y (2020). Management Considerations for Immune Checkpoint Inhibitor-Induced Enterocolitis Based on Management of Inflammatory Bowel Disease. Inflamm Bowel Dis 26, 662–668. - PubMed
-
- Andreae S, Piras F, Burdin N, and Triebel F (2002). Maturation and activation of dendritic cells induced by lymphocyte activation gene-3 (CD223). J Immunol 168, 3874–3880. - PubMed
-
- Arbour KC, Mezquita L, Long N, Rizvi H, Auclin E, Ni A, Martinez-Bernal G, Ferrara R, Lai WV, Hendriks LEL, et al. (2018). Impact of Baseline Steroids on Efficacy of Programmed Cell Death-1 and Programmed Death-Ligand 1 Blockade in Patients With Non-Small-Cell Lung Cancer. J Clin Oncol 36, 2872–2878. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
