

De Novo vs Acute-on-Chronic Presentations of Heart Failure-Related Cardiogenic Shock: Insights from the Critical Care Cardiology Trials Network Registry
- PMID: 34625127
- PMCID: PMC8514080
- DOI: 10.1016/j.cardfail.2021.08.014
De Novo vs Acute-on-Chronic Presentations of Heart Failure-Related Cardiogenic Shock: Insights from the Critical Care Cardiology Trials Network Registry
Abstract
Background: Heart failure-related cardiogenic shock (HF-CS) accounts for an increasing proportion of cases of CS in contemporary cardiac intensive care units. Whether the chronicity of HF identifies distinct clinical profiles of HF-CS is unknown.
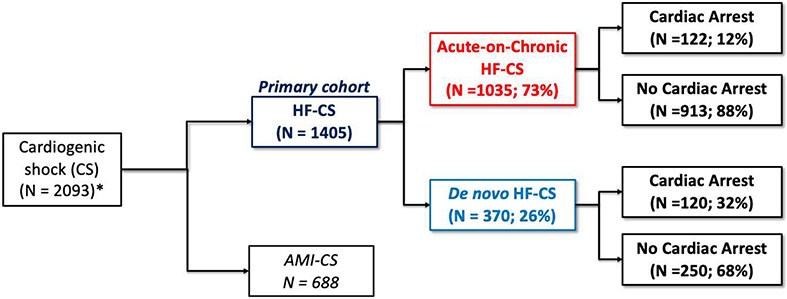
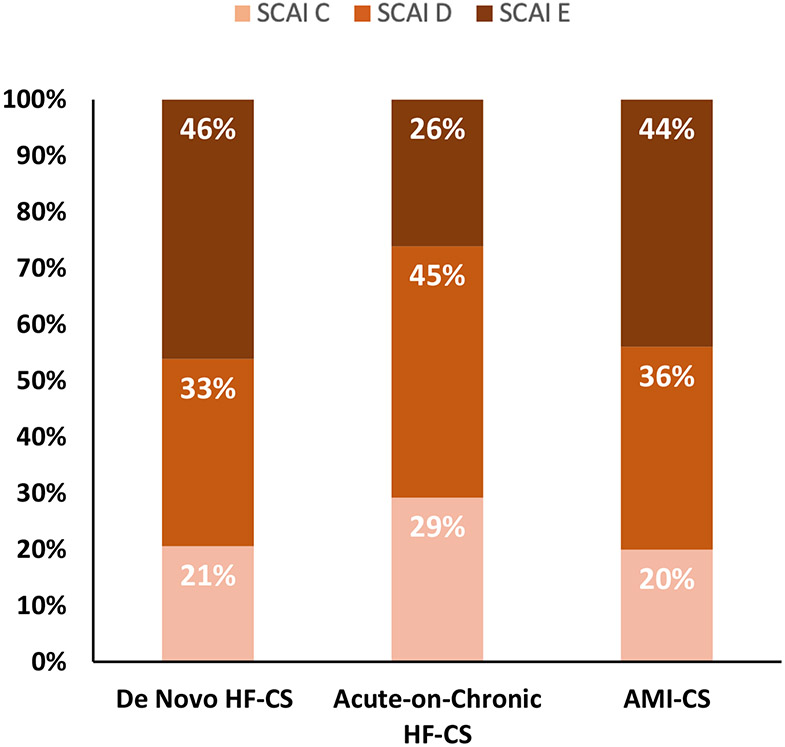
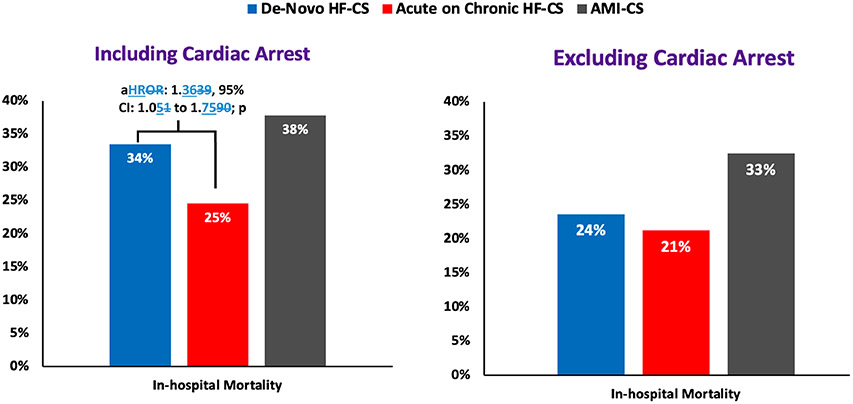
Methods and results: We evaluated admissions to cardiac intensive care units for HF-CS in 28 centers using data from the Critical Care Cardiology Trials Network registry (2017-2020). HF-CS was defined as CS due to ventricular failure in the absence of acute myocardial infarction and was classified as de novo vs acute-on-chronic based on the absence or presence of a prior diagnosis of HF, respectively. Clinical features, resource use, and outcomes were compared among groups. Of 1405 admissions with HF-CS, 370 had de novo HF-CS (26.3%), and 1035 had acute-on-chronic HF-CS (73.7%). Patients with de novo HF-CS had a lower prevalence of hypertension, diabetes, coronary artery disease, atrial fibrillation, and chronic kidney disease (all P < 0.01). Median Sequential Organ Failure Assessment (SOFA) scores were higher in those with de novo HF-CS (8; 25th-75th: 5-11) vs acute-on-chronic HF-CS (6; 25th-75th: 4-9, P < 0.01), as was the proportion of Society of Cardiovascular Angiography and Intervention (SCAI) shock stage E (46.1% vs 26.1%, P < 0.01). After adjustment for clinical covariates and preceding cardiac arrest, the risk of in-hospital mortality was higher in patients with de novo HF-CS than in those with acute-on-chronic HF-CS (adjusted hazard ratio 1.36, 95% confidence interval 1.05-1.75, P = 0.02).
Conclusions: Despite having fewer comorbidities, patients with de novo HF-CS had more severe shock presentations and worse in-hospital outcomes. Whether HF disease chronicity is associated with time-dependent compensatory adaptations, unique pathobiological features and responses to treatment in patients presenting with HF-CS warrants further investigation.
Keywords: cardiogenic shock; critical care cardiology; heart failure.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- Reynolds HR, Hochman JS. Cardiogenic shock: current concepts and improving outcomes. Circulation 2008; 117: 686–97. - PubMed
-
- Jentzer JC, Ahmed AM, Vallabhajosyula S, et al. Shock in the cardiac intensive care unit: Changes in epidemiology and prognosis over time. Am Heart J; 232: 94–104. - PubMed
-
- Harjola V-P, Lassus J, Sionis A, et al. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur J Heart Fail 2015; 17: 501–9. - PubMed
-
- van Diepen S, Katz JN, Albert NM, et al. Contemporary management of cardiogenic shock: A scientific statement from the american heart association. Circulation 2017; 136: e232–68. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
