Acute kidney injury in patients treated with immune checkpoint inhibitors
- PMID: 34625513
- PMCID: PMC8496384
- DOI: 10.1136/jitc-2021-003467
Acute kidney injury in patients treated with immune checkpoint inhibitors
Erratum in
-
Correction: Acute kidney injury in patients treated with immune checkpoint inhibitors.J Immunother Cancer. 2023 Apr;11(4):e003467corr1. doi: 10.1136/jitc-2021-003467corr1. J Immunother Cancer. 2023. PMID: 37094989 Free PMC article. No abstract available.
Abstract
Background: Immune checkpoint inhibitor-associated acute kidney injury (ICPi-AKI) has emerged as an important toxicity among patients with cancer.
Methods: We collected data on 429 patients with ICPi-AKI and 429 control patients who received ICPis contemporaneously but who did not develop ICPi-AKI from 30 sites in 10 countries. Multivariable logistic regression was used to identify predictors of ICPi-AKI and its recovery. A multivariable Cox model was used to estimate the effect of ICPi rechallenge versus no rechallenge on survival following ICPi-AKI.
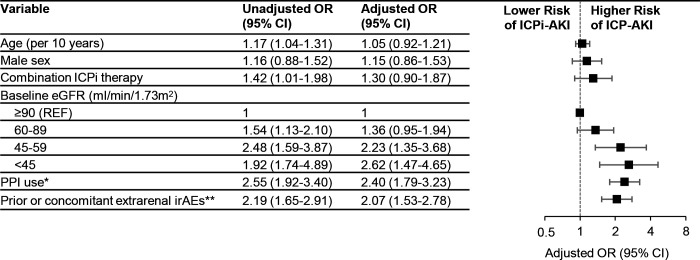
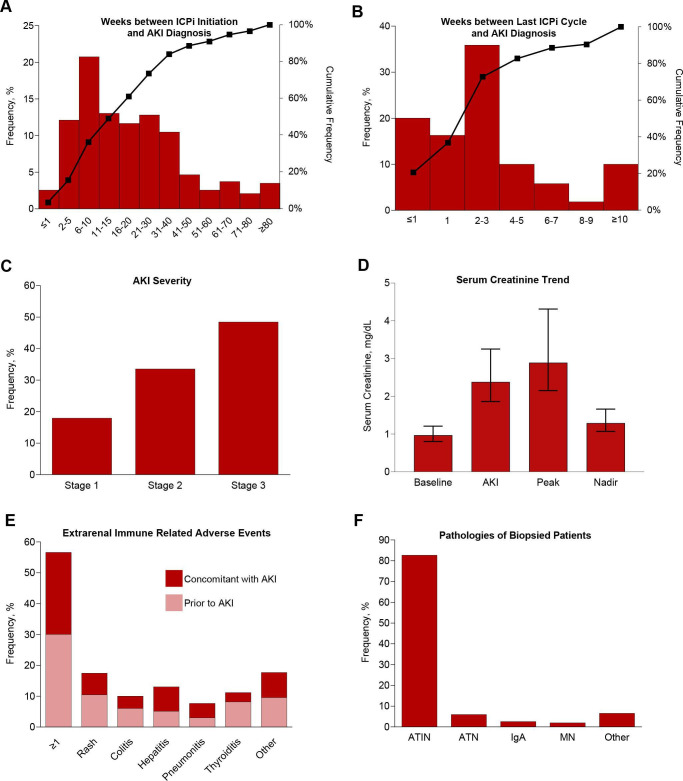
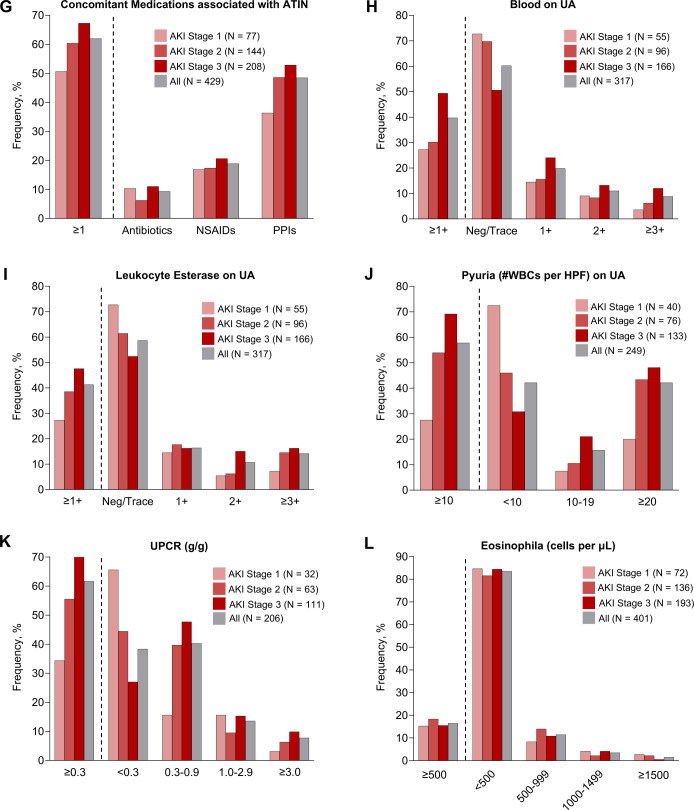
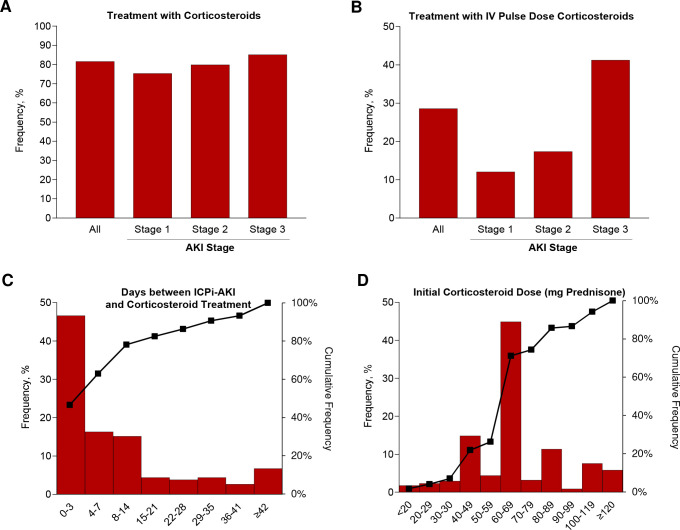
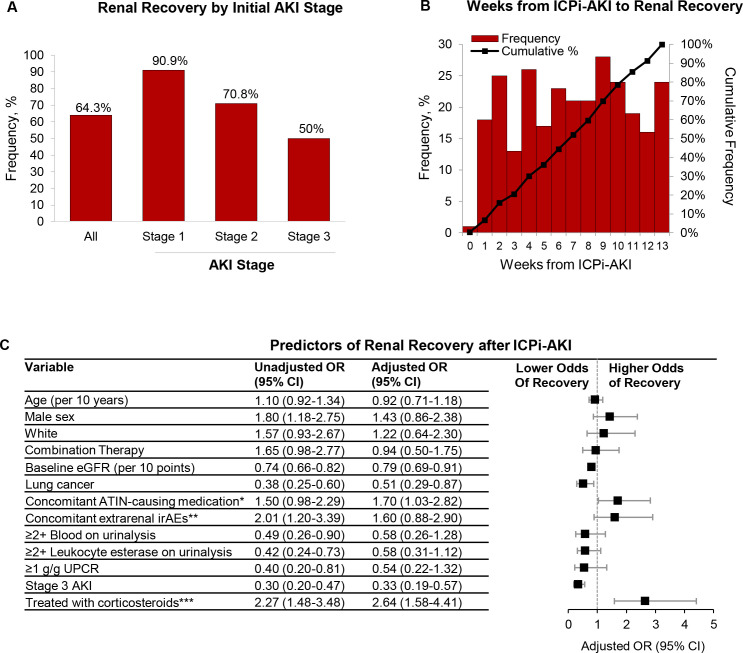
Results: ICPi-AKI occurred at a median of 16 weeks (IQR 8-32) following ICPi initiation. Lower baseline estimated glomerular filtration rate, proton pump inhibitor (PPI) use, and extrarenal immune-related adverse events (irAEs) were each associated with a higher risk of ICPi-AKI. Acute tubulointerstitial nephritis was the most common lesion on kidney biopsy (125/151 biopsied patients [82.7%]). Renal recovery occurred in 276 patients (64.3%) at a median of 7 weeks (IQR 3-10) following ICPi-AKI. Treatment with corticosteroids within 14 days following ICPi-AKI diagnosis was associated with higher odds of renal recovery (adjusted OR 2.64; 95% CI 1.58 to 4.41). Among patients treated with corticosteroids, early initiation of corticosteroids (within 3 days of ICPi-AKI) was associated with a higher odds of renal recovery compared with later initiation (more than 3 days following ICPi-AKI) (adjusted OR 2.09; 95% CI 1.16 to 3.79). Of 121 patients rechallenged, 20 (16.5%) developed recurrent ICPi-AKI. There was no difference in survival among patients rechallenged versus those not rechallenged following ICPi-AKI.
Conclusions: Patients who developed ICPi-AKI were more likely to have impaired renal function at baseline, use a PPI, and have extrarenal irAEs. Two-thirds of patients had renal recovery following ICPi-AKI. Treatment with corticosteroids was associated with improved renal recovery.
Keywords: CTLA-4 antigen; immunotherapy; programmed cell death 1 receptor.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Figures