

All-cause mortality and disease progression in SARS-CoV-2-infected patients with or without antibiotic therapy: an analysis of the LEOSS cohort
- PMID: 34625912
- PMCID: PMC8500268
- DOI: 10.1007/s15010-021-01699-2
All-cause mortality and disease progression in SARS-CoV-2-infected patients with or without antibiotic therapy: an analysis of the LEOSS cohort
Erratum in
-
Correction to: All-cause mortality and disease progression in SARS-CoV-2-infected patients with or without antibiotic therapy: an analysis of the LEOSS cohort.Infection. 2022 Apr;50(2):437-438. doi: 10.1007/s15010-021-01727-1. Infection. 2022. PMID: 34913136 Free PMC article. No abstract available.
Abstract
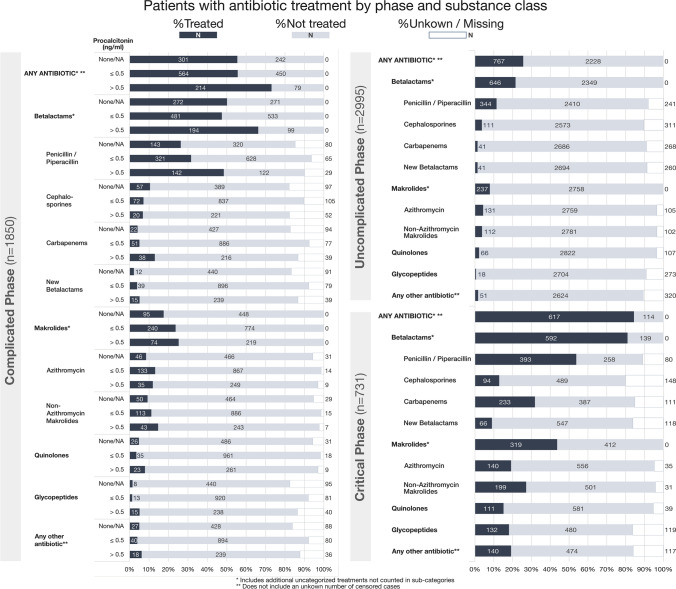
Purpose: Reported antibiotic use in coronavirus disease 2019 (COVID-19) is far higher than the actual rate of reported bacterial co- and superinfection. A better understanding of antibiotic therapy in COVID-19 is necessary.
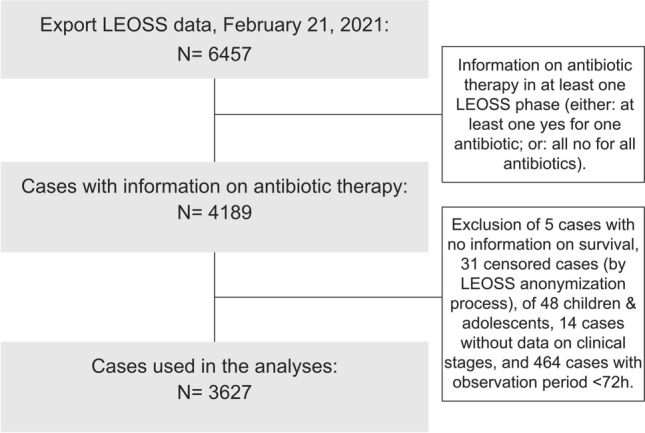
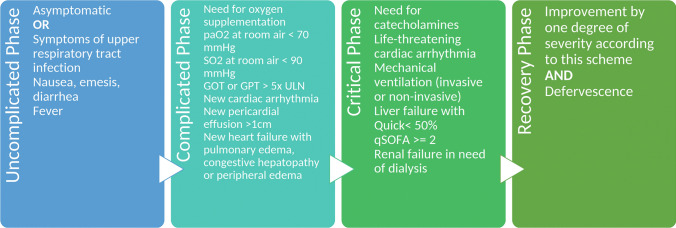
Methods: 6457 SARS-CoV-2-infected cases, documented from March 18, 2020, until February 16, 2021, in the LEOSS cohort were analyzed. As primary endpoint, the correlation between any antibiotic treatment and all-cause mortality/progression to the next more advanced phase of disease was calculated for adult patients in the complicated phase of disease and procalcitonin (PCT) ≤ 0.5 ng/ml. The analysis took the confounders gender, age, and comorbidities into account.
Results: Three thousand, six hundred twenty-seven cases matched all inclusion criteria for analyses. For the primary endpoint, antibiotic treatment was not correlated with lower all-cause mortality or progression to the next more advanced (critical) phase (n = 996) (both p > 0.05). For the secondary endpoints, patients in the uncomplicated phase (n = 1195), regardless of PCT level, had no lower all-cause mortality and did not progress less to the next more advanced (complicated) phase when treated with antibiotics (p > 0.05). Patients in the complicated phase with PCT > 0.5 ng/ml and antibiotic treatment (n = 286) had a significantly increased all-cause mortality (p = 0.029) but no significantly different probability of progression to the critical phase (p > 0.05).
Conclusion: In this cohort, antibiotics in SARS-CoV-2-infected patients were not associated with positive effects on all-cause mortality or disease progression. Additional studies are needed. Advice of local antibiotic stewardship- (ABS-) teams and local educational campaigns should be sought to improve rational antibiotic use in COVID-19 patients.
Keywords: Antibiotic stewardship; Antibiotics; COVID-19; LEOSS; Procalcitonin.
© 2021. The Author(s).
Conflict of interest statement
The authors do not disclose any conflicts of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
